Vous aimerez peut-être aussi
- Health Justice Now: Single Payer and What Comes NextD'EverandHealth Justice Now: Single Payer and What Comes NextÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)
- Health, Hope, and Healing for All: Toward More Equitable and Affordable HealthcareD'EverandHealth, Hope, and Healing for All: Toward More Equitable and Affordable HealthcarePas encore d'évaluation
- A Doctor’S Prescription for Health Care Reform: The National Medical Association Tackles Disparities, Stigma, and the Status QuoD'EverandA Doctor’S Prescription for Health Care Reform: The National Medical Association Tackles Disparities, Stigma, and the Status QuoPas encore d'évaluation
- The Nursing Home Decision: Easing the Transition for EveryoneD'EverandThe Nursing Home Decision: Easing the Transition for EveryonePas encore d'évaluation
- Healing Histories: Stories from Canada's Indian HospitalsD'EverandHealing Histories: Stories from Canada's Indian HospitalsPas encore d'évaluation
- Summary of Grown Woman Talk by Sharon Malone: Your Guide to Getting and Staying HealthyD'EverandSummary of Grown Woman Talk by Sharon Malone: Your Guide to Getting and Staying HealthyPas encore d'évaluation
- From the Family Doctor to the Current Disaster of Corporate Health Maintenance: How to Get Back to Real Patient Care!D'EverandFrom the Family Doctor to the Current Disaster of Corporate Health Maintenance: How to Get Back to Real Patient Care!Pas encore d'évaluation
- Remembering 2020: Year of the Most Memorable National ChallengesD'EverandRemembering 2020: Year of the Most Memorable National ChallengesPas encore d'évaluation
- A Grand Slam Life: A Physician Gets Covid, Finds His Way, and Works to Transform a Texas CommunityD'EverandA Grand Slam Life: A Physician Gets Covid, Finds His Way, and Works to Transform a Texas CommunityPas encore d'évaluation
- It’s Only a Bump: Overcoming Challenges in a Small-Town Medical PracticeD'EverandIt’s Only a Bump: Overcoming Challenges in a Small-Town Medical PracticeÉvaluation : 5 sur 5 étoiles5/5 (1)
- Turn Medicaid Nightmares into Miracles: Let's Deal with Medicaid and Protect Your Assets - Now!D'EverandTurn Medicaid Nightmares into Miracles: Let's Deal with Medicaid and Protect Your Assets - Now!Pas encore d'évaluation
- The Hidden Gifts of Helping: How the Power of Giving, Compassion, and Hope Can Get Us Through Hard TimesD'EverandThe Hidden Gifts of Helping: How the Power of Giving, Compassion, and Hope Can Get Us Through Hard TimesPas encore d'évaluation
- Convergence: The Marriage of Eastern and Western MedicineD'EverandConvergence: The Marriage of Eastern and Western MedicinePas encore d'évaluation
- Winning In The Last Inning: How to Grow Old, Stay Independent and Financially SolventD'EverandWinning In The Last Inning: How to Grow Old, Stay Independent and Financially SolventPas encore d'évaluation
- The Patient, The Doctor and The Bill Collector: An Obama Care and Medical Debt Collections Survival GuideD'EverandThe Patient, The Doctor and The Bill Collector: An Obama Care and Medical Debt Collections Survival GuidePas encore d'évaluation
- Ex-Acute: A Former Hospital Ceo Tells All on What’S Wrong with American HealthcareD'EverandEx-Acute: A Former Hospital Ceo Tells All on What’S Wrong with American HealthcarePas encore d'évaluation
- Our Health Plan: Community Governed Healthcare That WorksD'EverandOur Health Plan: Community Governed Healthcare That WorksPas encore d'évaluation
- Ultraprevention: The 6-Week Plan That Will Make You Healthy for LifeD'EverandUltraprevention: The 6-Week Plan That Will Make You Healthy for LifeÉvaluation : 3.5 sur 5 étoiles3.5/5 (15)
- Necessary Symbiosis: What Happens When Science and Government Work Together (and When They Don't)D'EverandNecessary Symbiosis: What Happens When Science and Government Work Together (and When They Don't)Pas encore d'évaluation
- Care: How People of Faith Can Respond to Our Broken Health SystemD'EverandCare: How People of Faith Can Respond to Our Broken Health SystemPas encore d'évaluation
- Riverview Hospital for Children and Youth: A Culture of PromiseD'EverandRiverview Hospital for Children and Youth: A Culture of PromisePas encore d'évaluation
- Deep Nutrition: Why Your Genes Need Traditional FoodD'EverandDeep Nutrition: Why Your Genes Need Traditional FoodÉvaluation : 4 sur 5 étoiles4/5 (51)
- The 2030 Caregiving Crisis: A Heavy Burden for Boomer ChildrenD'EverandThe 2030 Caregiving Crisis: A Heavy Burden for Boomer ChildrenPas encore d'évaluation
- Prime Example: The True Story of the Case that Saved Alternative Medicine in New York StateD'EverandPrime Example: The True Story of the Case that Saved Alternative Medicine in New York StatePas encore d'évaluation
- Authentic Health: The Definitive Guide to Losing Weight, Feeling Better, Mastering Stress, Sleeping Well Every Night, & Enjoying a Sense of PurposeD'EverandAuthentic Health: The Definitive Guide to Losing Weight, Feeling Better, Mastering Stress, Sleeping Well Every Night, & Enjoying a Sense of PurposePas encore d'évaluation
- My Mother, Your Mother: What to Expect As Parents AgeD'EverandMy Mother, Your Mother: What to Expect As Parents AgeÉvaluation : 4.5 sur 5 étoiles4.5/5 (12)
- Mountains Beyond Mountains Kathryn CrimDocument6 pagesMountains Beyond Mountains Kathryn Crimapi-579320483Pas encore d'évaluation
- Radical Charity: How Generosity Can Save the World (And the Church)D'EverandRadical Charity: How Generosity Can Save the World (And the Church)Pas encore d'évaluation
- The Poverty Industry: The Exploitation of America's Most Vulnerable CitizensD'EverandThe Poverty Industry: The Exploitation of America's Most Vulnerable CitizensÉvaluation : 3.5 sur 5 étoiles3.5/5 (7)
- Medication A.R.E.A.S. Bundle: A Prescription for Value-Based Healthcare to Optimize Patient Health Outcomes, Reduce Total Costs, and Improve Quality and Organization PerformanceD'EverandMedication A.R.E.A.S. Bundle: A Prescription for Value-Based Healthcare to Optimize Patient Health Outcomes, Reduce Total Costs, and Improve Quality and Organization PerformancePas encore d'évaluation
- Aging Well: Solutions to the Most Pressing Global Challenges of AgingD'EverandAging Well: Solutions to the Most Pressing Global Challenges of AgingPas encore d'évaluation
- Kwento Ni RosarioDocument3 pagesKwento Ni RosarioGrace Vidal0% (1)
- Your Dollars at Work: Success StoriesDocument16 pagesYour Dollars at Work: Success Storiesanon-812190Pas encore d'évaluation
- Dashboard: On The Road in Burangi KenyaDocument5 pagesDashboard: On The Road in Burangi KenyagenesisworldmissionPas encore d'évaluation
- Camp Constitution 2022 in ReviewDocument33 pagesCamp Constitution 2022 in ReviewHal ShurtleffPas encore d'évaluation
- Deep StateDocument145 pagesDeep StateHal Shurtleff100% (3)
- Critical Race Theory PresentationDocument18 pagesCritical Race Theory PresentationHal ShurtleffPas encore d'évaluation
- COVID 19 and The Agendas To Come Red Pilled Slides Part 2Document36 pagesCOVID 19 and The Agendas To Come Red Pilled Slides Part 2Hal ShurtleffPas encore d'évaluation
- Agenda 21 Slide Deck by Hal ShurtleffDocument134 pagesAgenda 21 Slide Deck by Hal ShurtleffCamp Constitution's Scribd Page100% (3)
- Deep StateDocument145 pagesDeep StateHal Shurtleff100% (3)
- COVID 19 and The Agendas To Come Red Pilled Slides Part 1Document36 pagesCOVID 19 and The Agendas To Come Red Pilled Slides Part 1Hal ShurtleffPas encore d'évaluation
- Camp Constitution Reading HourDocument3 pagesCamp Constitution Reading HourHal ShurtleffPas encore d'évaluation
- Communist Attack On JBSDocument16 pagesCommunist Attack On JBSHal Shurtleff100% (1)
- Donation Form To Support Camp ConstitutionDocument1 pageDonation Form To Support Camp ConstitutionHal ShurtleffPas encore d'évaluation
- Camp Constitution Power Point PresentationDocument42 pagesCamp Constitution Power Point PresentationHal ShurtleffPas encore d'évaluation
- Memorial of The Inauguration of The Statue of Franklin N. B. ShurtleffDocument449 pagesMemorial of The Inauguration of The Statue of Franklin N. B. ShurtleffHal ShurtleffPas encore d'évaluation
- Documents of The City of Boston With Nathaniel B. Shurtleff's Innagural Address Jan 6, 1869Document1 065 pagesDocuments of The City of Boston With Nathaniel B. Shurtleff's Innagural Address Jan 6, 1869Hal ShurtleffPas encore d'évaluation
- John Birch Society Press Clipping in New England From 1990 To 2015.Document161 pagesJohn Birch Society Press Clipping in New England From 1990 To 2015.Hal ShurtleffPas encore d'évaluation
- Vietnam War Petition DriveDocument2 pagesVietnam War Petition DriveHal ShurtleffPas encore d'évaluation
- A National Constitutional Convention and Its Possible ConsequencesDocument12 pagesA National Constitutional Convention and Its Possible ConsequencesHal ShurtleffPas encore d'évaluation
- ModelCon ConStateRescissionResolution2011Document1 pageModelCon ConStateRescissionResolution2011lgreenleyPas encore d'évaluation
- Weston - Sampson - Heritage Rail Trail Feasibility Study - 1 22 16 Dedham, MA Agenda 21, ICLEIDocument28 pagesWeston - Sampson - Heritage Rail Trail Feasibility Study - 1 22 16 Dedham, MA Agenda 21, ICLEIHal ShurtleffPas encore d'évaluation
- History of The Town of Carver MassachuseDocument505 pagesHistory of The Town of Carver MassachuseHal ShurtleffPas encore d'évaluation
- Turkey - Author of Genocide (1965)Document32 pagesTurkey - Author of Genocide (1965)Hal ShurtleffPas encore d'évaluation
- Abortion A Dogma in Search of A RationaleDocument8 pagesAbortion A Dogma in Search of A RationaleHal ShurtleffPas encore d'évaluation
- The Communist Attack On US PoliceDocument116 pagesThe Communist Attack On US PoliceHal Shurtleff100% (1)
- Letter To State Legislators EverywhereDocument4 pagesLetter To State Legislators EverywhereHal ShurtleffPas encore d'évaluation
- "The Truth About The Confederate Battle Flag "By Pastor John WeaverDocument36 pages"The Truth About The Confederate Battle Flag "By Pastor John WeaverHal ShurtleffPas encore d'évaluation
- Letter To Sam Blumenfeld From Lee EdwardsDocument1 pageLetter To Sam Blumenfeld From Lee EdwardsHal ShurtleffPas encore d'évaluation
- A Flyer Promoting The Greater Boston John Birch Society's 2015 Christmas Breakfast Saturday Dec 12, 2015Document1 pageA Flyer Promoting The Greater Boston John Birch Society's 2015 Christmas Breakfast Saturday Dec 12, 2015Hal ShurtleffPas encore d'évaluation
- Dangers of An Article V Convention Lyndonville, VTDocument2 pagesDangers of An Article V Convention Lyndonville, VTHal ShurtleffPas encore d'évaluation
- Execute The Laws To Restore The Republic Presentation in Thomaston, ME Wednesday October 15, 2014Document2 pagesExecute The Laws To Restore The Republic Presentation in Thomaston, ME Wednesday October 15, 2014Hal ShurtleffPas encore d'évaluation
- Introduction To Psychiatric Nursing: Module 2: ConceptsDocument26 pagesIntroduction To Psychiatric Nursing: Module 2: ConceptsJoric MagusaraPas encore d'évaluation
- Sample Lesson PlanDocument6 pagesSample Lesson PlanChristian Geo MolinaPas encore d'évaluation
- DOH Devolution Transition PlanDocument32 pagesDOH Devolution Transition PlanMichi Go100% (1)
- A Healthy ImageDocument6 pagesA Healthy Imagedwi yolla OkhesiaPas encore d'évaluation
- CHN FinalsDocument6 pagesCHN FinalsSHERMINA HASANPas encore d'évaluation
- Size, Density, Composition, Rate of Growth, Mobility, Social Class and Educational LevelDocument2 pagesSize, Density, Composition, Rate of Growth, Mobility, Social Class and Educational Levelczeremar chanPas encore d'évaluation
- 修改版Document5 pages修改版Eris LPas encore d'évaluation
- 2013 - A BJÖRKDAHL - Theinfluenceofstafftrainingontheviolenceprevention (Retrieved-2014!11!04)Document9 pages2013 - A BJÖRKDAHL - Theinfluenceofstafftrainingontheviolenceprevention (Retrieved-2014!11!04)fairwoodsPas encore d'évaluation
- Skills FCPDocument3 pagesSkills FCPPauline AñesPas encore d'évaluation
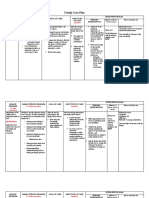
- Nursing Care PlanDocument2 pagesNursing Care PlanIrish Paping TucyapaoPas encore d'évaluation
- 11aug2023 - Advertisement For Direct Recruitment of Non Teaching Staff - Nurses and Others - LevelDocument14 pages11aug2023 - Advertisement For Direct Recruitment of Non Teaching Staff - Nurses and Others - Levelakashrathor19115Pas encore d'évaluation
- Clinical Nursing Skills 8th Edition Smith Test BankDocument10 pagesClinical Nursing Skills 8th Edition Smith Test Banktracybrownfmaczqejxw100% (9)
- Guidelines For Recruitment IDocument2 pagesGuidelines For Recruitment IAnonymous yyWma2Pas encore d'évaluation
- PHINMA Education NetworkDocument3 pagesPHINMA Education NetworkMichelle Dona MirallesPas encore d'évaluation
- NRLS 0236 Wristbands SPN 2005 11 22 v1Document6 pagesNRLS 0236 Wristbands SPN 2005 11 22 v1irene damanikPas encore d'évaluation
- PB Nursing I - July 014Document11 pagesPB Nursing I - July 014bibekananda87Pas encore d'évaluation
- New FileDocument10 pagesNew FileTrí VănPas encore d'évaluation
- Future Direction For Client Education: Group 3Document19 pagesFuture Direction For Client Education: Group 3Rheal P Esmail100% (1)
- Origins of Nursing & Nursing ReformsDocument30 pagesOrigins of Nursing & Nursing ReformsSuleiman KikulwePas encore d'évaluation
- Nursing Care Plan - MRSADocument4 pagesNursing Care Plan - MRSAKasiban MuniandyPas encore d'évaluation
- Advisory Guidance - Administration of Medicines by Nursing AssociatesDocument16 pagesAdvisory Guidance - Administration of Medicines by Nursing AssociatesMaggiePas encore d'évaluation
- CARingDocument37 pagesCARingvetra melania sinagaPas encore d'évaluation
- Occupational Health and Safety Issues Among Nurses in The PhilippinesDocument4 pagesOccupational Health and Safety Issues Among Nurses in The PhilippinesDani CawaiPas encore d'évaluation
- Poster Abstract Book PDFDocument804 pagesPoster Abstract Book PDFRyan Michael OducadoPas encore d'évaluation
- 300 Items QuestionnaireDocument62 pages300 Items Questionnairestuffednurse100% (5)
- Managemnet MCQDocument6 pagesManagemnet MCQKhushi Khushi100% (1)
- Measuring Workload of Icu Nurses With A Questionnaire Survey The Nasa Task Load Index (TLX)Document22 pagesMeasuring Workload of Icu Nurses With A Questionnaire Survey The Nasa Task Load Index (TLX)Fathur RahmatPas encore d'évaluation
- Perioperative Nursing Lecture Week 1 Day 1 PDFDocument29 pagesPerioperative Nursing Lecture Week 1 Day 1 PDFKimberlie Dela Merced TomasPas encore d'évaluation
- Significance and Beneficiaries of StudyDocument22 pagesSignificance and Beneficiaries of StudyJehu Rey Obrero CabañesPas encore d'évaluation
- Nursing Practice IIIDocument17 pagesNursing Practice IIIstuffednurse100% (3)