Vous aimerez peut-être aussi
- Clinical Handbook of Cardiac ElectrophysiologyD'EverandClinical Handbook of Cardiac ElectrophysiologyBenedict M. GloverPas encore d'évaluation
- Case-Based Device Therapy for Heart FailureD'EverandCase-Based Device Therapy for Heart FailureUlrika Birgersdotter-GreenPas encore d'évaluation
- Kallergis 2012Document9 pagesKallergis 2012fairuzPas encore d'évaluation
- Ecg ManfestationsDocument19 pagesEcg Manfestationsnaxo128Pas encore d'évaluation
- AV Bloc Induces TDPDocument13 pagesAV Bloc Induces TDPMirza AlfiansyahPas encore d'évaluation
- Roden Understanding Prolongation QT Anda Cancer Therapy 2019Document29 pagesRoden Understanding Prolongation QT Anda Cancer Therapy 2019Cardiologia NeumologiaPas encore d'évaluation
- Electrocardiograma en TóxicologiaDocument19 pagesElectrocardiograma en TóxicologiaLaura GPas encore d'évaluation
- Literature Review 2019Document15 pagesLiterature Review 2019Р. МөнхжинPas encore d'évaluation
- Genetic Biomarkers For The Risk of Seizures in Long QT SyndromeDocument9 pagesGenetic Biomarkers For The Risk of Seizures in Long QT SyndromeР. МөнхжинPas encore d'évaluation
- Drug-Induced QT Interval ProlongationDocument13 pagesDrug-Induced QT Interval ProlongationgeoaislaPas encore d'évaluation
- Long QT and Torsades NuevoDocument17 pagesLong QT and Torsades NuevoAnel ConquetPas encore d'évaluation
- Long QT Syndrome: Diagnosis and Management: BackgroundDocument8 pagesLong QT Syndrome: Diagnosis and Management: BackgroundArizkie AlfiPas encore d'évaluation
- Prevalence and Clinical Correlates of QT Prolongation in Patients With Hypertrophic CardiomyopathyDocument7 pagesPrevalence and Clinical Correlates of QT Prolongation in Patients With Hypertrophic CardiomyopathyNITACORDEIROPas encore d'évaluation
- NIH Public Access: Author ManuscriptDocument4 pagesNIH Public Access: Author ManuscriptaudiPas encore d'évaluation
- Poster: Cardiac Adverse Reactions Associated With Psychotropic DrugsDocument4 pagesPoster: Cardiac Adverse Reactions Associated With Psychotropic Drugsandi aprizalPas encore d'évaluation
- MEDSCAPE ACCOUNT QT - Association of Antipsychotic and Antidepressant Drugs With Q-T Interval ProlongationDocument11 pagesMEDSCAPE ACCOUNT QT - Association of Antipsychotic and Antidepressant Drugs With Q-T Interval ProlongationHesbon MomanyiPas encore d'évaluation
- Long QT SyndromeDocument9 pagesLong QT SyndromeRoberto SalazarPas encore d'évaluation
- Genetic Case 1Document44 pagesGenetic Case 1blue pianoPas encore d'évaluation
- Antz Elev ItchDocument12 pagesAntz Elev ItchAdrianaPas encore d'évaluation
- Article 1Document4 pagesArticle 1Fakhar Mahmood ShahidPas encore d'évaluation
- Managing Drug-Induced QT Prolongation in ClinicalDocument7 pagesManaging Drug-Induced QT Prolongation in ClinicalDewi AmeliaPas encore d'évaluation
- How To Detect Long QT in A Heartbeat - Clinical ViewDocument9 pagesHow To Detect Long QT in A Heartbeat - Clinical ViewAlberto MHPas encore d'évaluation
- Mohebi 2017Document26 pagesMohebi 2017Ioana GuțăPas encore d'évaluation
- Circulation 2002 Wu 675 6Document3 pagesCirculation 2002 Wu 675 6konyekPas encore d'évaluation
- Cocaine Related Torsade de Pointes in A Methadone Maintenance PatientDocument9 pagesCocaine Related Torsade de Pointes in A Methadone Maintenance Patientgene flowersPas encore d'évaluation
- 1 s2.0 S0749070421001020 MainDocument12 pages1 s2.0 S0749070421001020 MainEliseu AmaralPas encore d'évaluation
- 99591Document7 pages99591jimejuanfePas encore d'évaluation
- Chapter 32 - Genetic Cardiac ArrythmiasDocument7 pagesChapter 32 - Genetic Cardiac ArrythmiasReda SoPas encore d'évaluation
- General Practitioner, Cardiologist, Mimika General Hospital, Central Papua, IndonesiaDocument5 pagesGeneral Practitioner, Cardiologist, Mimika General Hospital, Central Papua, IndonesiafillygogoPas encore d'évaluation
- Criem2020 4159526Document5 pagesCriem2020 4159526m.fahimsharifiPas encore d'évaluation
- QT Dispersion Increases During Hemodialysis With Low-Calcium DialysateDocument6 pagesQT Dispersion Increases During Hemodialysis With Low-Calcium Dialysatebryan chanPas encore d'évaluation
- long-QT Syndrome Epinephrine Unmasks Latent Mutation Carriers With LQT1 Form of CongenitalDocument12 pageslong-QT Syndrome Epinephrine Unmasks Latent Mutation Carriers With LQT1 Form of Congenitalapi-26166949Pas encore d'évaluation
- Therapeutic Implications: Short QT Syndrome: Clinical Findings and DiagnosticDocument8 pagesTherapeutic Implications: Short QT Syndrome: Clinical Findings and DiagnosticNITACORDEIROPas encore d'évaluation
- Mujer Con Torsades de PointesDocument2 pagesMujer Con Torsades de PointesAníbal José Arroyo RodríguezPas encore d'évaluation
- Ventricular Tachyarrhythmias: Roger D. White, M.DDocument2 pagesVentricular Tachyarrhythmias: Roger D. White, M.DEugene VovchukPas encore d'évaluation
- The QT Interval PDFDocument4 pagesThe QT Interval PDFFeliciaSetiawanPas encore d'évaluation
- ECG Frequency Changes inDocument13 pagesECG Frequency Changes inArief KamilPas encore d'évaluation
- TIA: Transient Ischemic Attack Key PointsDocument2 pagesTIA: Transient Ischemic Attack Key PointsAlmahira Az ZahraPas encore d'évaluation
- Muerte Subita en DMDocument10 pagesMuerte Subita en DMChristian Morejon QuezadaPas encore d'évaluation
- R On T PhenomeneonDocument3 pagesR On T Phenomeneonpradeep danielPas encore d'évaluation
- Leading Article Quinolone-Induced QT Interval Prolongation: A Not-So-Unexpected Class EffectDocument4 pagesLeading Article Quinolone-Induced QT Interval Prolongation: A Not-So-Unexpected Class EffectHà Trần ThanhPas encore d'évaluation
- Current Trends in Supraventricular Tachycardia Management: Daniel Sohinki, MD, Owen A. Obel, MDDocument10 pagesCurrent Trends in Supraventricular Tachycardia Management: Daniel Sohinki, MD, Owen A. Obel, MDAffandi HafidPas encore d'évaluation
- Extract Analysis T-Waves ECG Atrial Flutter VinetDocument9 pagesExtract Analysis T-Waves ECG Atrial Flutter VinetAlex WongPas encore d'évaluation
- SCD - Investigations & - CausesDocument29 pagesSCD - Investigations & - Causesasna0% (1)
- Arritmias Cardiacas Inducidas Por AntibioticosDocument7 pagesArritmias Cardiacas Inducidas Por AntibioticosIrving Torres LópezPas encore d'évaluation
- Increasingly Sensitive Assays For Cardiac TroponinsDocument8 pagesIncreasingly Sensitive Assays For Cardiac TroponinsAbel Espinoza MedallaPas encore d'évaluation
- Hiperkalemia 1 PDFDocument5 pagesHiperkalemia 1 PDFablfilaPas encore d'évaluation
- VT 2Document49 pagesVT 2Micija CucuPas encore d'évaluation
- Patofisiologi and Clinical Manifest LQTSDocument9 pagesPatofisiologi and Clinical Manifest LQTSNonamePas encore d'évaluation
- ABC of Clinical Electrocardiography Myocardial IschaemiaDocument6 pagesABC of Clinical Electrocardiography Myocardial IschaemiaShri Mahalaxmi HarishPas encore d'évaluation
- How To Diagnose The Cause of Sudden Cardiac ArrestDocument7 pagesHow To Diagnose The Cause of Sudden Cardiac ArrestTaufik Muhammad JrPas encore d'évaluation
- Follow-Up of 316 Molecularly Defined Pediatric Long-QT Syndrome PatientsDocument9 pagesFollow-Up of 316 Molecularly Defined Pediatric Long-QT Syndrome PatientsР. МөнхжинPas encore d'évaluation
- When Past Is Prologue: Clinical Problem-SolvingDocument7 pagesWhen Past Is Prologue: Clinical Problem-SolvingJoni WitziPas encore d'évaluation
- Dong 2022Document8 pagesDong 2022Olivia LimPas encore d'évaluation
- ECG Predictors of Sudden Cardiac Death in Cardiomyopathies: Yoga Yuniadi Indonesian Heart Rhythm SocietyDocument27 pagesECG Predictors of Sudden Cardiac Death in Cardiomyopathies: Yoga Yuniadi Indonesian Heart Rhythm SocietyCarissa CkPas encore d'évaluation
- QT SyndromeDocument7 pagesQT SyndromeRikhardo RkPas encore d'évaluation
- Journal Homepage: - : IntroductionDocument12 pagesJournal Homepage: - : IntroductionIJAR JOURNALPas encore d'évaluation
- 2018 - Manifestaciones Electrocardiograficas de La Hiperkalemia SeveraDocument4 pages2018 - Manifestaciones Electrocardiograficas de La Hiperkalemia SeveraNANDY LUZ FERIA DIAZPas encore d'évaluation
- 1 s2.0 S2666084923003509 MainDocument6 pages1 s2.0 S2666084923003509 MainThato PaulusPas encore d'évaluation
- PIIS0007091217355952Document9 pagesPIIS0007091217355952Said Qadaru APas encore d'évaluation
- Medico-Legal Issues in AnaesthesiaDocument2 pagesMedico-Legal Issues in AnaesthesiaSuresh KumarPas encore d'évaluation
- GO S For Tamilnadu DoctorsDocument160 pagesGO S For Tamilnadu DoctorsSuresh KumarPas encore d'évaluation
- Ventilator Associated Pneumonia (Vap)Document11 pagesVentilator Associated Pneumonia (Vap)Suresh KumarPas encore d'évaluation
- Local Anaesthetic AgentsDocument21 pagesLocal Anaesthetic AgentsSuresh KumarPas encore d'évaluation
- Anaesthetic Management of Blunt Chest TraumaDocument11 pagesAnaesthetic Management of Blunt Chest TraumaSuresh KumarPas encore d'évaluation
- Spinal Anesthesia For Caeserian Section: Comparison of 5.0% Lignocaine and 0.5% BupivacaineDocument4 pagesSpinal Anesthesia For Caeserian Section: Comparison of 5.0% Lignocaine and 0.5% BupivacaineSuresh KumarPas encore d'évaluation
- Perioperative Management of A Patient With Left Ventricular FailureDocument6 pagesPerioperative Management of A Patient With Left Ventricular FailureSuresh KumarPas encore d'évaluation
- Controversial Issues in NeuroanaesthesiaDocument12 pagesControversial Issues in NeuroanaesthesiaSuresh KumarPas encore d'évaluation
- Cerebral Protection What Is New ?Document11 pagesCerebral Protection What Is New ?Suresh Kumar100% (1)
- Alleviating Cancer PainDocument9 pagesAlleviating Cancer PainSuresh KumarPas encore d'évaluation
- Anaesthesia Care Beyond Operating Rooms: Newer Opportunities & Challenges.Document8 pagesAnaesthesia Care Beyond Operating Rooms: Newer Opportunities & Challenges.Suresh Kumar100% (1)
- Anaesthetic Management of Ihd Patients For Non Cardiac SurgeryDocument18 pagesAnaesthetic Management of Ihd Patients For Non Cardiac SurgerySuresh KumarPas encore d'évaluation
- Day Care AnesthesiaDocument4 pagesDay Care AnesthesiaSuresh KumarPas encore d'évaluation
- Anaesthesia in The Gastrointestinal Endoscopy SuiteDocument3 pagesAnaesthesia in The Gastrointestinal Endoscopy SuiteSuresh KumarPas encore d'évaluation
- Depth of Anesthesia & MonitoringDocument2 pagesDepth of Anesthesia & MonitoringSuresh KumarPas encore d'évaluation
- Role of The Anaesthesiologists in The Management of BurnsDocument12 pagesRole of The Anaesthesiologists in The Management of BurnsSuresh KumarPas encore d'évaluation
- Surgical Patients at Risk For Renal FailureDocument35 pagesSurgical Patients at Risk For Renal FailureSuresh KumarPas encore d'évaluation
- Muscle Relaxants in Current PracticeDocument6 pagesMuscle Relaxants in Current PracticeSuresh KumarPas encore d'évaluation
- Anaesthetic Management of Bleeding Obstetric PatientDocument10 pagesAnaesthetic Management of Bleeding Obstetric PatientSuresh KumarPas encore d'évaluation
- Labour Analgesia - Recent ConceptsDocument18 pagesLabour Analgesia - Recent ConceptsSuresh KumarPas encore d'évaluation
- Preoperative Anaesthetic Risk Assessment and Risk Reduction Before SurgeryDocument17 pagesPreoperative Anaesthetic Risk Assessment and Risk Reduction Before SurgerySuresh KumarPas encore d'évaluation
- Anaesthetic Management of Patients With Pacemakers and Implantable Cardioverter Defibrillator.Document16 pagesAnaesthetic Management of Patients With Pacemakers and Implantable Cardioverter Defibrillator.Suresh KumarPas encore d'évaluation
- Anaesthesia For Bleeding TonsilDocument6 pagesAnaesthesia For Bleeding TonsilSave MedicalEducation Save HealthCarePas encore d'évaluation
- Anesthesia For Fetal SurgeryDocument8 pagesAnesthesia For Fetal SurgerySuresh KumarPas encore d'évaluation
- Pre-Operative Cardio-Pulmonary Exercise Testing (Cpet)Document14 pagesPre-Operative Cardio-Pulmonary Exercise Testing (Cpet)Suresh KumarPas encore d'évaluation
- Fluid Resuscitation in TraumaDocument17 pagesFluid Resuscitation in TraumaSuresh Kumar100% (1)
- Analysis of Arterial Blood GasesDocument17 pagesAnalysis of Arterial Blood GasesSuresh KumarPas encore d'évaluation
- Pulmonary Function Test in Pre Anaesthetic EvaluationDocument10 pagesPulmonary Function Test in Pre Anaesthetic EvaluationSuresh KumarPas encore d'évaluation
- Anaesthesia Breathing SystemsDocument15 pagesAnaesthesia Breathing SystemsSuresh KumarPas encore d'évaluation
- Basic Physics Applied To AnaesthesiologyDocument10 pagesBasic Physics Applied To AnaesthesiologySuresh KumarPas encore d'évaluation
- Tank Emission Calculation FormDocument12 pagesTank Emission Calculation FormOmarTraficanteDelacasitosPas encore d'évaluation
- Eclipsecon MQTT Dashboard SessionDocument82 pagesEclipsecon MQTT Dashboard Sessionoscar.diciomma8446Pas encore d'évaluation
- Fact Pack Financial Services KenyaDocument12 pagesFact Pack Financial Services KenyaCatherinePas encore d'évaluation
- SVPWM PDFDocument5 pagesSVPWM PDFmauricetappaPas encore d'évaluation
- Oasis 360 Overview 0710Document21 pagesOasis 360 Overview 0710mychar600% (1)
- Prepositions Below by in On To of Above at Between From/toDocument2 pagesPrepositions Below by in On To of Above at Between From/toVille VianPas encore d'évaluation
- Well Stimulation TechniquesDocument165 pagesWell Stimulation TechniquesRafael MorenoPas encore d'évaluation
- Chapter 1 Hospital and Clinical Pharmacy Choplete PDF Notes D.Pharma 2nd Notes PDF NoteskartsDocument7 pagesChapter 1 Hospital and Clinical Pharmacy Choplete PDF Notes D.Pharma 2nd Notes PDF NoteskartsDrx Brajendra LodhiPas encore d'évaluation
- 01 Eh307 Crimpro Case Digests Part 1Document214 pages01 Eh307 Crimpro Case Digests Part 1Kimberly PerezPas encore d'évaluation
- Pediatric Skills For OT Assistants 3rd Ed.Document645 pagesPediatric Skills For OT Assistants 3rd Ed.Patrice Escobar100% (1)
- Pharaoh TextDocument143 pagesPharaoh Textanon_31362848Pas encore d'évaluation
- IBMC Competition Booklet 2013Document40 pagesIBMC Competition Booklet 2013Rollins Center at BYUPas encore d'évaluation
- BS en 118-2013-11Document22 pagesBS en 118-2013-11Abey VettoorPas encore d'évaluation
- La Bugal-b'Laan Tribal Association Et - Al Vs Ramos Et - AlDocument6 pagesLa Bugal-b'Laan Tribal Association Et - Al Vs Ramos Et - AlMarlouis U. PlanasPas encore d'évaluation
- R 18 Model B Installation of TC Auxiliary Lights and WingletsDocument29 pagesR 18 Model B Installation of TC Auxiliary Lights and WingletsAlejandro RodríguezPas encore d'évaluation
- Rules On Evidence PDFDocument35 pagesRules On Evidence PDFEuodia HodeshPas encore d'évaluation
- How Can You Achieve Safety and Profitability ?Document32 pagesHow Can You Achieve Safety and Profitability ?Mohamed OmarPas encore d'évaluation
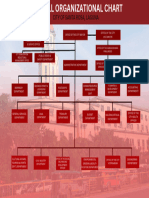
- Org ChartDocument1 pageOrg Chart2021-101781Pas encore d'évaluation
- U2 - Week1 PDFDocument7 pagesU2 - Week1 PDFJUANITO MARINOPas encore d'évaluation
- Software Testing Notes Prepared by Mrs. R. Swetha M.E Unit I - Introduction at The End of This Unit, The Student Will Be Able ToDocument30 pagesSoftware Testing Notes Prepared by Mrs. R. Swetha M.E Unit I - Introduction at The End of This Unit, The Student Will Be Able ToKabilan NarashimhanPas encore d'évaluation
- Flyer Manuale - CON WATERMARK PAGINE SINGOLEDocument6 pagesFlyer Manuale - CON WATERMARK PAGINE SINGOLEjscmtPas encore d'évaluation
- CEC Proposed Additional Canopy at Guard House (RFA-2021!09!134) (Signed 23sep21)Document3 pagesCEC Proposed Additional Canopy at Guard House (RFA-2021!09!134) (Signed 23sep21)MichaelPas encore d'évaluation
- Land Use Paln in La Trinidad BenguetDocument19 pagesLand Use Paln in La Trinidad BenguetErin FontanillaPas encore d'évaluation
- Fcode 54 en El SytucDocument2 pagesFcode 54 en El SytucAga MenonPas encore d'évaluation
- Best Practices in Developing High PotentialsDocument9 pagesBest Practices in Developing High PotentialsSuresh ShetyePas encore d'évaluation
- Safety Inspection Checklist Project: Location: Inspector: DateDocument2 pagesSafety Inspection Checklist Project: Location: Inspector: Dateyono DaryonoPas encore d'évaluation
- Finaniial AsceptsDocument280 pagesFinaniial AsceptsKshipra PrakashPas encore d'évaluation
- CPM W1.1Document19 pagesCPM W1.1HARIJITH K SPas encore d'évaluation
- Completed NGC3 ReportDocument4 pagesCompleted NGC3 ReportTiCu Constantin100% (1)
- Computer System Sevicing NC Ii: SectorDocument44 pagesComputer System Sevicing NC Ii: SectorJess QuizzaganPas encore d'évaluation