Vous aimerez peut-être aussi
- Bacterial ToxinsDocument25 pagesBacterial ToxinsA. PathakPas encore d'évaluation
- Simple Colloid GoitreDocument7 pagesSimple Colloid GoitreA. Pathak50% (2)
- Hypersensitivity ReactionsDocument66 pagesHypersensitivity ReactionsA. PathakPas encore d'évaluation
- Coins by Dr. H.D. PathakDocument17 pagesCoins by Dr. H.D. PathakA. PathakPas encore d'évaluation
- Pleomorphic Adenoma of Parotid GlandDocument14 pagesPleomorphic Adenoma of Parotid GlandA. Pathak100% (1)
- Giant Cell Tumor or OsteoclastomaDocument6 pagesGiant Cell Tumor or OsteoclastomaA. PathakPas encore d'évaluation
- Tuberculous LymphadenitisDocument16 pagesTuberculous LymphadenitisA. PathakPas encore d'évaluation
- Fibroadenoma of BreastDocument7 pagesFibroadenoma of BreastA. PathakPas encore d'évaluation
- Squamous Cell CarcinomaDocument12 pagesSquamous Cell CarcinomaA. Pathak0% (1)
- Adenocarcinoma of BreastDocument7 pagesAdenocarcinoma of BreastA. PathakPas encore d'évaluation
- MeningitisDocument65 pagesMeningitisA. Pathak100% (7)
- Immune SystemDocument145 pagesImmune SystemA. Pathak100% (9)
- Auto ImmunityDocument44 pagesAuto ImmunityA. PathakPas encore d'évaluation
- Rare Coins From UJJAINDocument18 pagesRare Coins From UJJAINA. Pathak100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Application Form Health Examination Form Parents Consent FormDocument1 pageApplication Form Health Examination Form Parents Consent Formapril rose catainaPas encore d'évaluation
- 1 s2.0 S0223523417309327 MainDocument12 pages1 s2.0 S0223523417309327 MainDan NechitaPas encore d'évaluation
- Hla IgDocument48 pagesHla Igprakas44Pas encore d'évaluation
- Cobas Ampliprep Cobas TaqMan HCV Viral LoadDocument84 pagesCobas Ampliprep Cobas TaqMan HCV Viral LoadMolecular_Diagnostics_KKUHPas encore d'évaluation
- Avian Preventive Medicine Recommended BooksDocument17 pagesAvian Preventive Medicine Recommended BooksFarhan NobelPas encore d'évaluation
- Mesenchymal Stem Cell Therapeutic Intervention in Covid19Document9 pagesMesenchymal Stem Cell Therapeutic Intervention in Covid19Bala BhaskarPas encore d'évaluation
- Clinical Microbiology Reviews-2006-Scollard-338.full PDFDocument44 pagesClinical Microbiology Reviews-2006-Scollard-338.full PDFBogdan FuereaPas encore d'évaluation
- Doctor Interviews Documentaries & Research QuotesDocument32 pagesDoctor Interviews Documentaries & Research QuotesjdhPas encore d'évaluation
- Gastritis Englis 2018Document115 pagesGastritis Englis 2018irinaPas encore d'évaluation
- Week-12 VirologyDocument8 pagesWeek-12 VirologyAlex LiganPas encore d'évaluation
- Know Your Hospital - A Guide To Getting The Best CareDocument9 pagesKnow Your Hospital - A Guide To Getting The Best CareMike PosktovaPas encore d'évaluation
- Chapter 22 Upper Respiratory DisorderDocument171 pagesChapter 22 Upper Respiratory DisorderAnnette Aquino GuevarraPas encore d'évaluation
- Kumpulan Soal Transfusi DarahDocument6 pagesKumpulan Soal Transfusi DarahdrnyolPas encore d'évaluation
- Catalogue of Potato Varieties and Advanced Clones 2011Document2 pagesCatalogue of Potato Varieties and Advanced Clones 2011cip-libraryPas encore d'évaluation
- Aplastic AnemiaDocument13 pagesAplastic AnemiaHazel Eñga Tiam WatPas encore d'évaluation
- Introduction To MicrobiologyDocument35 pagesIntroduction To MicrobiologytoobanaeemPas encore d'évaluation
- Idr 177247 Healthcare Associated Infections An Overview 111418Document13 pagesIdr 177247 Healthcare Associated Infections An Overview 111418ednihs100% (1)
- SBI Recording FormsDocument9 pagesSBI Recording FormsElmalyn BernartePas encore d'évaluation
- Americanas Neumo PDFDocument291 pagesAmericanas Neumo PDFUri MoraPas encore d'évaluation
- Biology Practical Part 2Document23 pagesBiology Practical Part 2jiya singh100% (2)
- Daftar PustakaDocument2 pagesDaftar Pustakacute_chooeyPas encore d'évaluation
- Escaping The Era of Pandemics': Experts Warn Worse Crises To Come Options Offered To Reduce RiskDocument96 pagesEscaping The Era of Pandemics': Experts Warn Worse Crises To Come Options Offered To Reduce RiskComunicarSe-ArchivoPas encore d'évaluation
- Self LigationDocument2 pagesSelf Ligationdavidrocks81Pas encore d'évaluation
- Emirates Pre Employment Medical Examination Form PDFDocument9 pagesEmirates Pre Employment Medical Examination Form PDFLoredana Marin100% (1)
- DSFDSFDSFDSFDocument108 pagesDSFDSFDSFDSFbarzulkakPas encore d'évaluation
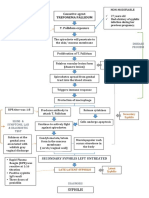
- Path o Physiology of SyphilisDocument1 pagePath o Physiology of Syphilis3S - JOCSON, DENESE NICOLE LEE M.Pas encore d'évaluation
- Community Health NursingDocument78 pagesCommunity Health NursingJagveer ChauhanPas encore d'évaluation
- MicrobiologyDocument17 pagesMicrobiologykimacol659Pas encore d'évaluation
- Rheumatic Fever: Assoc - Prof.Dr - Zurkurnai Yusof USMDocument25 pagesRheumatic Fever: Assoc - Prof.Dr - Zurkurnai Yusof USMfadlicardio100% (1)
- Nose, Sinuses, Mouth, and LarynxDocument3 pagesNose, Sinuses, Mouth, and LarynxjottowagPas encore d'évaluation