SPECIAL ARTICLES
Neuropsychiatric
Complications of
Efavirenz Therapy:
Suggestions for a New
Research Paradigm
Stefan Sütterlin, Dipl.-Psych.
Claus Vögele, Ph.D.
Siegfried Gauggel, Ph.D.
This review gives an up-to-date account of the
current state of research on neuropsychiatric E favirenz is a commonly used non-nucleoside re-
verse transcriptase inhibitor frequently prescribed
in combination with other antiretroviral regimens (e.g.,
complications associated with efavirenz therapy
and critiques the methods used in previous stud- protease inhibitors) for the treatment of HIV. After its
admission for pharmaceutical treatment in the United
ies. The authors suggest an extension of current
States in 1998, efavirenz has become a cornerstone for
research strategies using psychophysiological con-
highly active antiretroviral therapies (HAART). Good
cepts and including behavioral regulation models. CNS penetration has been seen as a major strength of
From a practical perspective, these may contrib- antiretroviral regimens, particularly efavirenz. Accu-
ute to better screening methods for the identifica- mulating evidence suggests neuroprotective effects
tion of those at risk for neuropsychiatric compli- against cognitive decline such as HIV-associated de-
cations and the improvement of neuropsychiatric mentia and other aspects of neuropsychological func-
monitoring during efavirenz treatment. From a tioning.1–4 Nevertheless, its proven effectiveness as a
theoretical viewpoint, the suggested research first-line treatment in suppressing plasma viral load
paradigms may help to move beyond the cur- comes along with reports of adverse central-nervous
rent state of descriptive approaches and thus and neuropsychiatric effects which have been fre-
improve our limited understanding of underly- quently reported after exposure to efavirenz.5–9
ing mechanisms.
Types and Prevalence Rates of Efavirenz-Associated
(The Journal of Neuropsychiatry and Clinical
Neuropsychiatric Effects: Current Evidence
Neurosciences 2010; 22:361–369)
Depression, suicidal ideation, aggressive/impulsive be-
havior, paranoid reactions, manic reactions and (largely
Received May 19, 2009; revised August 13 and September 30, 2009;
accepted October 5, 2009. Mr. Sütterlin and Dr. Vögele are affiliated
with the Research Unit INSIDE at the University of Luxembourg;
Dr. Gauggel is affiliated with the Institute of Medical Psychology and
Medical Sociology at RWTH Aachen University, in Aachen, North
Rhine-Westphalia, Germany. Address correspondence to Stefan
Sütterlin, Dipl.-Psych., University of Luxembourg, Research Unit
INSIDE, Building XII, Room 201C, Route de Diekirch, L-7220
Walferdange, Luxembourg; Stefan.Suetterlin@uni.lu (e-mail).
Copyright © 2010 American Psychiatric Publishing, Inc.
J Neuropsychiatry Clin Neurosci 22:4, Fall 2010 http://neuro.psychiatryonline.org 361
NEUROPSYCHIATRIC COMPLICATIONS OF EFAVIRENZ THERAPY
anecdotal reports of) psychosis-like behavior, suicide, edly confirmed in numerous controlled trials, these
and severe delusions are among the most frequently data refer to the incremental contribution of risk, which
reported psychiatric symptoms associated with efa- cannot be explained by HIV-associated long-term brain
virenz treatment. Dizziness, insomnia, impaired con- damage. In direct comparison to treatment alternatives,
centration, irritability, nervousness, somnolence, abnor- adverse effects resulting from treatments including efa-
mal dreams, and hallucinations are usually classified as virenz are reported three times more often than in cases
CNS symptoms. The differentiation between CNS- of protease inhibitors.7
related and psychiatric symptoms is rather arbitrary In terms of symptom manifestation over time, the
and has not been consistent; in general, psychiatric most severe toxicity effects of efavirenz treatment are
symptoms include some sort of behavioral or conscious consistently reported to occur within the first 2– 4 weeks
component. This differentiation aims to reflect differ- after efavirenz initiation,7 and symptoms generally
ences at the symptom level but does not necessarily cease after 6 – 8 weeks.5,9 Long-term effects covering
imply distinct causal mechanisms. periods of more than 12 weeks after efavirenz treatment
Estimates of prevalence rates have varied over the onset have rarely been investigated. Following a prag-
years in line with the progress of efavirenz toxicity matic approach, studies have usually focused on clini-
research, from early anecdotal case reports10 –15 and cally relevant symptoms that could impact on medica-
cross-sectional controlled trials16 –18 to prospective tion adherence rather than the investigation of causal
studies of larger samples19 and a growing number of pathways of the reported adverse reactions. Conse-
reviews.5–7,9 Recent studies have focused on the rel- quently, most studies prioritized the application of as-
evance of plasma concentrations and genetic predis- sessment tools and research designs suitable for the
positions as moderators of neuropsychiatric compli- diagnosis of mental disorders rather than the identifi-
cations.20 –25 cation of subclinical symptoms.
The Food and Drug Administration8 reported results Subsequent research has reported mild and clinically
from a sample of 1,008 patients with HIV who received tolerable persistent impairments of psychological func-
treatment with efavirenz, and it stated the probability of tioning for up to 2 years after treatment onset.16 The
“selected nervous-system symptoms of any severity” Efavirenz Consensus Working Group and other re-
regardless of causality as 52.7% compared with 24.6% in searchers29,30 published recommendations for the treat-
a control group (HIV⫹ individuals not receiving efa- ment of efavirenz-induced adverse effects, including
virenz). The risk of discontinuation of treatment as a psychopharmacological treatment as well as nonphar-
result of experiencing symptoms was 2.1% in efavirenz- macological symptom-specific management strategies
treated patients compared with 1.1% in the control such as psychotherapeutic treatment.
group. On average, prevalence rates range from 40% to
70%.15,26 –28 This wide range in prevalence estimates is Methodological Shortcomings in Previous Research
probably due to differences in study design (e.g., sam- Research on efavirenz treatment-associated neuropsy-
ple sizes, recruitment methods, and assessment of neu- chiatric toxicity suffers from a range of methodological
ropsychiatric complications) and methodological qual- shortcomings, which have rarely been addressed in pre-
ity, but it is also due to the inconsistent use of terms vious reviews. First, studies have often neglected the
such as “CNS-related toxicity,” “psychiatric,” and assessment of a psychiatric baseline status, often due to
“neuropsychiatric,” and categorizing mental disorders their retrospective design.31 Occasionally, interviewees
such as major depression or posttraumatic stress disor- were asked to provide a retrospective report on their
der using unspecified diagnostic criteria. To complicate mental status before treatment.32 In neither of the pub-
the picture further, few studies have used assessment lished prospective studies was a psychiatric, psycholog-
tools that are suitable for detecting efavirenz treatment- ical, or neuropsychological baseline status before efa-
associated complications on a subclinical level. Taking virenz treatment onset statistically controlled for,
into account such methodological differences in early although psychiatric history is considered a relevant
publications on efavirenz toxicity, reports on preva- predictor for neuropsychiatric effects triggered by efa-
lence rates have since converged and remain relatively virenz. Second, the few published prospective studies
stable; an average of one out of two patients receiving suffer from high attrition rates and are thus very likely
efavirenz shows adverse psychiatric reactions. Repeat- to underestimate the prevalence of psychiatric disor-
362 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 22:4, Fall 2010
SÜTTERLIN et al.
ders in the actual outcome of clinical trials.27 This un- viral therapy leads to early improvements in motor-
derestimation is caused by selection biases and the related tasks impairs the interpretational power of
likely association of poor adherence and psychiatric dis- the results in terms of neuropsychological function-
orders at treatment onset, which is often not assessed. ing.
Third, assessments in the form of semistructured inter- von Giesen et al.31 used the “Kurztest zur Erfassung
views were applied by either researchers not blinded to von Gedächtnis- und Aufmerksamkeitsleistungen”
the treatment condition (e.g., prescribing physicians), (Short Test for the Assessment of Memory and Atten-
those without suitable training in the conduct of the tion Performance). This is a screening tool designed to
interview, or both.19 Fourth, in the vast majority of detect early dementia without sufficient differentiation
studies, nonstandardized assessment tools were used or of memory and attention. It is, thus, insensitive to subtle
measures applied that are insensitive for the detection or moderate changes in cognitive function related to
of prodromal symptoms.16,31,32 efavirenz treatment, especially when compared to HIV
While the almost exclusive use of self-report mea- patients not receiving efavirenz but likely to show HIV-
sures in previous studies has enabled the identification related impairments. In addition, assessors were not
of clinically important symptoms, their lack of specific- blinded to the treatment condition. The study is, there-
ity in relation to neurophysiological pathways does not fore, methodically flawed, and its results (91% of par-
allow for any conclusions to be drawn about the mech- ticipants scored 0, “no severe cognitive impairment”)
anisms linking efavirenz and neuropsychiatric compli- are probably due to a floor effect. The authors’ conclu-
cations. In addition, assessment tools such as screening sion that “the present data do not provide evidence for
tests and symptom checklists appear to be too insensitive a higher incidence of light and/or severe neuropsychi-
and too global to detect symptoms at the subclinical level. atric side effects” (p. 382) associated with efavirenz
These assessments are, therefore, likely to result in type II treatment is, therefore, questionable and unsupported
error, particularly in monitoring more subtle long-term by their evidence.
effects. Statistical power, effect sizes, or both were rarely In summary, no extensive or theory-driven neuropsy-
reported, though this information would be crucial in or- chological assessment has been attempted in studies on
der to adequately assess the appropriateness of the ap- efavirenz toxicity. Current conclusions regarding neu-
plied assessment procedures and the severity of adverse ropsychological performance have to be considered
reactions in samples that range from single case studies to premature and largely unsupported by evidence.
large cohorts. Following a bottom-up approach, recent research
A particularly striking omission from previous re- has investigated the influence of the G516T polymor-
search investigating efavirenz treatment-associated side phism at the CYP2B6 isoenzyme on intracellular efa-
effects concerns the almost complete lack of appropriate virenz plasma levels and has identified a CYP2B6
neuropsychological assessments. The only published genotype as a predictor of efavirenz neuropsycholog-
and frequently cited studies claiming to have explicitly ical toxicity.23,25 Patients with a homozygotic 516G⬎T
investigated neuropsychological symptoms related to substitution show higher efavirenz plasma levels and
efavirenz treatment are those from Clifford et al.33 and report more frequent adverse reactions to efavirenz
von Giesen et al.31 Both studies conclude that neuro- treatment due to less effective intracellular drug clear-
psychological symptoms did not occur or were only ance compared with those carrying the wild type (GG).
mild and temporary. Nevertheless, the selection of These results could not be replicated in one other
subtests from standardized assessment tools was not study.22
theoretically justified in either study. For example, Nevertheless, the findings from Lowenhaupt et al.23
Clifford et al.33 used composite scores (“NPZ3”) that and Rotger et al.25 point to the possibility that previous
were inappropriately derived (adding subscores of investigations of efavirenz-related adverse effects may
Trail Making tests A and B to the total of its subscales), have suffered from low statistical power as they did not
omitted crucial neuropsychological domains, and were take into account inter-individual differences in drug
unspecific. These scores, therefore, do not allow for a clearance capacity. Drug clearance or efavirenz plasma
comprehensive assessment of the “neuropsychologi- levels are obvious moderators of any outcome in studies
cal status” of patients with HIV. Furthermore, the investigating toxicity associated with efavirenz treatment.
previously reported34 –37 observation that antiretro- Future research investigating causal pathways between
J Neuropsychiatry Clin Neurosci 22:4, Fall 2010 http://neuro.psychiatryonline.org 363
NEUROPSYCHIATRIC COMPLICATIONS OF EFAVIRENZ THERAPY
efavirenz treatment and its adverse side effects should, risk potential for future drugs taking effect in the
therefore, screen participants for carriers of the G516T CNS.
allele or include a measure of efavirenz clearance, or both,
in order to identify those subsamples with increased vul- Suggestion for a New Research Approach
nerability because of slow drug clearance. Previous research on efavirenz treatment-associated
neuropsychiatric toxicity has been largely descrip-
tive, with the aim to identify, classify, and assess the
Questions Unanswered by Current Research probability and severity of symptoms that may impair
Efavirenz is only one of several regimens in the class treatment adherence for this effective and daily admin-
of retroviral inhibitors. Nevertheless, its extraordinary istered lifelong medication. Despite considerable im-
effective penetration into the CNS and its unique ap- provements in risk management by including genotyp-
proach to the inhibition of viral reverse transcriptase have ing in medical decisions in vulnerable populations and
earned efavirenz the status of a first-line treatment despite recommendations for risk management strategies, the
its significantly higher risk of neurologic toxicity com- missing link between pathological symptoms and efa-
pared with other regimens of antiretroviral therapy. The virenz has not been identified yet. Current research,
reasons why neuropsychiatric effects occur more fre- therefore, is confined to providing practice guidelines
quently and with greater severity during efavirenz treat- for clinicians to maximize adherence rather than explor-
ment than, for example, during treatment with the struc- ing their origin (e.g., alternative treatment options, dose
turally comparable nevirapine6,7 remain unclear, as the reduction, prescription of antidepressants, and non-
identification of neural pathways and systems responsible pharmacological interventions).
for these adverse effects is still pending. We argue, therefore, for the development of a theory-
Early case studies from the late 1990s and conference driven and standardized way of screening for neuro-
contributions on toxicity related to efavirenz treat- psychiatric toxicities in efavirenz and other antiretrovi-
ment38 triggered a fast-growing pool of empirical data ral agents. We suggest a top-down approach by
feeding into early reviews on efavirenz toxicity,15 rec- classifying and integrating typical efavirenz-related
ommending the monitoring of CNS adverse effects in symptoms such as depression, suicidal ideation, aggres-
all patients taking efavirenz. Psychiatric diagnoses, sive/impulsive behavior, delusions, impaired concen-
however, often remained rather vague, with some pub- tration, irritability, and nervousness into the psycholog-
lications citing merely anecdotal observations without ical concept of self-regulation. This approach
using standardized assessment methods or specified complements existing bottom-up research strategies in
diagnostic criteria. There was a preponderance of prag- medical research and makes use of the profile of clinical
matic approaches in terms of risk management and the symptomatology associated with efavirenz treatment,
development of practice guidelines. Research designs indicating an impairment of functions which can
and their implications were, therefore, rarely discussed. largely be conceptualized as behavioral, cognitive and
This practice-oriented “bottom-up approach” can be affective dysregulation (Figure 1).
contrasted with a “top-down approach,” which links Concepts and methods from psychophysiology and ex-
the results on efavirenz treatment-associated symptoms perimental and clinical neuropsychology can locate cur-
with theoretical models from the behavioral sciences. rent results in a theoretical framework, which will gener-
Such an approach may contribute to a more compre- ate testable hypotheses that go beyond the selection of
hensive understanding of the complex interplay of cel- appropriate assessment tools. Such a model would allow
lular level mechanisms and behavioral patterns. for the identification of subtle effects of efavirenz on psy-
We argue that a shift in focus from clinical treat- chophysiological levels, leading to the identification of the
ment-related toxicities to the development of a con- neuronal networks affected. The similarities of efavirenz-
ceptual framework would allow for the improvement associated symptoms to syndromes observed in brain-
of screening methods for individuals at risk for ad- damaged patients with dysexecutive functions and their
verse reactions following efavirenz treatment. This involvement of systems of behavioral control suggest the
paradigm shift would also help to improve monitor- application of standard paradigms designed for neuro-
ing methods (early alerts) and contribute to the de- psychological profiling in patients with inhibition-related
velopment of tests applied to detect neuropsychiatric impairments.39 Results from the neurosciences and psy-
364 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 22:4, Fall 2010
SÜTTERLIN et al.
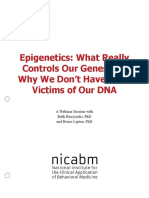
FIGURE 1. A New Research Paradigm for the Study of Efavirenz Treatment-Related Toxicities
Clinical symptoms of
behavioral, affective, and
cognitive dysregulation
ch
proa Subtle changes of
ap behavioral, affective,
wn
-do and cognitive regulation
d top
e ste
gg
Su Dysregulated
psychophysiological processes
of behavioral control
Screening,
Changes of activity in monitoring,
neuronal networks identifying of all
causal relations
Descriptive,
Cellular level effects
correlational research
of efavirenz basic research
approach
Pharmacogenetics
This theory-driven approach applies psychological models of behavioral regulation to observed manifestations of efavirenz treatment-
related toxicities. Psychophysiological concepts link the subjective and social perspective of human behavior and experience with
physiological correlates, which can be systematically assessed using standardized techniques. Empirical evidence for neuropsychological
underpinnings of psychophysiological phenomena provides theoretical connections to neuronal activity patterns resulting in maladaptive
behavior. A comprehensive approach making use of psychophysiological heuristics offers standardized and practical tools which might be
applied in screening, monitoring, and fundamental research.
chology have established the capacity to self-regulate be- vations with established psychophysiological research
havior, to resist impulses, and to regulate emotions effec- paradigms, the assessment of peripheral parameters
tively as a personality trait.40 Behavioral neuroscience of such as cardiac autonomic balance might contribute to
self-regulation links traditional psychological approaches a better understanding of behavioral dysregulation in
of behavioral theory with their neurological underpin- efavirenz-treated patients. The neuroanatomical con-
nings and implies standardized assessment tools for fine- cept of central autonomic networks44,45 depicts a pro-
grained analyses of cognitive and behavioral regulative cess of neurovisceral integration in which peripheral
skills and their neuronal substrates, basically located in psychophysiological reactions (heart rate, salivation,
the frontal cortex.41 Behavioral self-regulation is often un- electrodermal reactions, and startle reflex potentiation)
derstood as one of several functions within the broad and are related to neocortical structures such as the prefron-
sometimes fuzzy concept of executive functions. Research tal cortex (PFC) and cingulate cortex as well as subcor-
on dysexecutive syndromes provides models and specific tical limbic areas (thalamus, hypothalamus, and amyg-
experimental paradigms39 further supported by neuroim- dalae), triggering autonomic reactions. The degree of
aging techniques which have not been used in efavirenz- flexibility of this system is related to adaptive behavior,
related research on psychiatric or psychological adverse including complex behavioral processes such as social
effects.42,43 Neuropsychological and psychophysiological interaction. On a peripheral level, this is expressed by
research on self-regulation makes use of assessment tech- vagal tone. Reciprocal cortico-cardiac interactions are
niques that detect and quantify subtle neuronal and phys- key features of the central autonomic networks and are
iological processes relevant for behavioral control such as indicated by the sympathetic-parasympathetic inter-
frontal inhibitory functions. play as it is expressed in heart rate variability. Auto-
To give a more specific example for potentially inter- nomic nervous system-related measures such as heart
esting new research paradigms linking symptom obser- rate variability or baroreceptor sensitivity can be con-
J Neuropsychiatry Clin Neurosci 22:4, Fall 2010 http://neuro.psychiatryonline.org 365
NEUROPSYCHIATRIC COMPLICATIONS OF EFAVIRENZ THERAPY
ceived as a proxy for sympatho-vagal-balance, and due Symptomatic manifestations of dysregulated behavior
to their neuroanatomic relation to the PFC, they also typically following efavirenz toxicity suggest this meth-
indicate an individual’s self-regulative capacities.46,47 od’s relevance for possibly related symptoms for phar-
Observed deficits in behavioral regulation as de- macological treatment. The neural generators, which
scribed in cases of efavirenz-induced neuropsychiatric compose the N200 and the relevance of these anatomi-
reactions fit well into the psychological concepts of self- cal structures for behavioral and cognitive regulation,
regulation, which cognitive neuroscience interprets as are well researched. The same applies to other event-
behavioral correlates of executive functions associated related potentials occurring early or late over the time
with the PFC, the ventro-medial PFC, and the cingulate course. They indicate features of cognitive processing
cortex. These neuronal correlates and their correspond- and thus provide a quantitative assessment with much
ing autonomic functions, as predicted in central auto- higher temporal resolution than through solely behav-
nomic network theory, allow the deployment of estab- ioral observation, though their selection is based on
lished and standardized assessment tools. Hence, by self-report information.
applying new theory-driven research approaches, The methods outlined above are examples of stan-
drug-induced behavioral abnormalities can be illumi- dardized tools that assess behavioral and emotional
nated, screening methods improved, and treatment op- regulation. They have been shown to contribute to a bet-
tions considered. ter understanding of a variety of affective and behavioral
The concept of central autonomic networks empha- disorders covering the same class of symptoms of disin-
sizes the reciprocal interactions between (prefrontal) hibition as described in the literature on efavirenz side
cortical and cardiac processes and is in line with frontal effects (e.g., impulsivity,58 affective disorders,59,60 psycho-
hypofunction in patients who show symptoms of be- pathology in general44,61 and various other psychiatric
havioral, affective, or cognitive dysregulation. Making symptoms, impairments of executive functions,39,42,43,59
use of the reciprocity of the central-autonomic net- and cognitive performance62) (Table 1).
works, an exemplary application of this concept could Models of and empirical findings on executive func-
involve biofeedback of heart rate variability or respira- tions and their relation to frontal inhibition and behav-
tory sinus arrhythmia. This method is easy to use and ioral regulation42 can provide an extensive framework
has established efficacy in the treatment of depression48 for behavioral regulation. Such concepts link neuroana-
and anxiety disorders.49 The reciprocity of cortico-car- tomical structures and psychophysiological processes
diac interactions, based on cortical plasticity, provides with observable behavior in everyday life63,64 and en-
opportunities for behavioral interventions.50,51 able researchers to a theory-driven choice of specific
Electrophysiological correlates of behavior (e.g., and sensitive assessment methods.
event-related potentials) illuminate features of cogni- We hope this new research approach will help to
tive top-down and bottom-up processes such as evalu- improve guidelines for efavirenz treatment by provid-
ation, categorization, orienting/alertness, or novelty ing more sensitive assessment tools (i.e., those that are
and are sensitive to pharmacological treatments. Sev- able to detect subtle subclinical changes, thus enabling
eral features such as amplitude and latency of event- practitioners to prevent or minimize treatment-associ-
related potentials can be linked to behavioral or cogni- ated adverse effects). We further expect progress in
tive dysregulation. Response inhibition paradigms research on the identification of persons at risk for ad-
combine behavioral tasks requiring motor inhibition in verse effects of efavirenz treatment and argue for the
standardized and well-established paradigms such as introduction of paradigms developed in behavioral sci-
Go-NoGo,48,49 stop-signal,53 or others with correspond- ences to be applied in research on drug side effects with
ing electrophysiological measures such as N200 ampli- psychological and psychiatric implications.
tude.54 A sensitive measure such as the inhibition-re-
lated N200 event-related potential may be able to assess
subclinical changes in cognitive and behavioral regula- CONCLUSION
tion processes,55 which have been suggested to be based
on a supermodal inhibition-eliciting initiatior in the In this review we suggest a change in research para-
right inferior prefrontal cortex and, therefore, to be digms and conceptualize efavirenz-related side effects
closely linked to cognitive adaptivity and flexibility.56,57 as manifestations of behavioral dysregulation. We pro-
366 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 22:4, Fall 2010
SÜTTERLIN et al.
TABLE 1. Suggested Methodological Approaches for the Identification of Sub-Clinical Toxic Effects
Toxic Effects Data Level Exemplary Assessment Methods
Subtle changes of behavioral, affective Self-report of sub-clinical symptoms Standardized questionnaires for the assessment
and cognitive regulation in everyday context of prodromal symptoms in non-clinical
populations: e.g., CES-D, Barret Impulsivity
Scale, Behavior Rating Inventory of
Executive Function (BRIEF), etc.
Dysregulated psychophysiological Behavioral assessment and Response inhibition; Heart rate variability;
processes of behavioral control autonomic function electrodermal activity; distractibility and
attentional biases
Changes of activity patterns in Physiological assessment of CNS Event-related potentials (N100, N200, P3a/b,
neuronal networks functions of attention and etc.); frontal alpha-asymmetries
cognitive control
The suggested methodological approaches and assessment tools are only exemplary and can be extended. CES-D⫽Center for Epidemiologic
Studies Depression Scale
pose to extend current research strategies to a theory- The assessment methods suggested here are estab-
driven top-down process tying together existing knowl- lished and standardized; data for various common psy-
edge on self-regulation theory. Previous research on chological and psychiatric disorders frequently de-
efavirenz toxicity is restricted to purely descriptive ap- scribed as efavirenz-related adverse effects are
proaches at the symptom level. By suggesting a top- available. This will generate hypotheses for risk assess-
down, theory-driven strategy we argue for applying ment and risk management, screening methods, moni-
established and standardized assessment tools, which toring, and prescription criteria and opens new per-
are provided by the psychophysiological concepts of spectives for the investigation of neuronal networks
self-regulation. The aims of this reconceptualization are and pathways. We argue that the identification and
the improvement of screening methods for the identi- quantification of efavirenz treatment-related subtle and
fication of patients at risk for efavirenz treatment-re- subclinical changes on cognitive, behavioral, and emo-
lated side effects, the enhancement of fundamental re- tional levels are crucial for substantial progress from
search on self-regulation-related effects of purely descriptive approaches of the past toward an
pharmacological substances passing the blood-brain understanding of psychopharmacological effects. These
barrier, and the establishment of effective and close subtle changes require appropriate research designs
monitoring during treatment. This approach enables (controlled, double-blinded) and standardized assess-
researchers to tap into established knowledge in or- ment tools beyond behavioral observation and self-re-
der to choose specific and sensitive psychophysiolog- port in order to tap into existing knowledge of behav-
ical assessment tools based on hypotheses derived ioral regulation and its origins. This approach and its
from observation and self-reports of previous re- related methodology address serious limitations in cur-
search. The use of psychophysiological measures in rent research by bridging the gap between fundamental
the assessment process enables the quantification of research in neurobiological domains and behavioral sci-
treatment-related side effects with high temporal so- ences.
lution, comparative measurements, and sensitivity
toward subclinical effects, and thus provides a new This paper has benefitted in its early stages from discus-
source of information. sions with Dr. Rupert Whitaker, Tuke Institute, London.
References
1. Cysique LA, Vaida F, Letendre S, et al: Dynamics of cogni- 4. Wynn HE, Brundage RC, Fletcher CV: Clinical implications of CNS
tive change in impaired HIV-positive patients initiating an- penetration of antiretroviral drugs. CNS Drugs 2002; 16:595–609
tiretroviral therapy. Neurology 2009; 73:342–348 5. Arendt G, de Nocker D, Giesen HJ, et al: Neuropsychiatric
2. Liner KJ, Hall CD, Robertson KR: Effects of antiretroviral therapy side effects of efavirenz therapy. Expert Opin Drug Saf 2007;
on cognitive impairment. Curr HIV/AIDS Reports 2008; 5:64 –71 6:147–154
3. Pollicita M, Aquaro S, Svicher V, et al: HIV-1-associated de- 6. Barreiro P, Garcı́a-Benayas T, Soriano V, et al: Simplification of
mentia during HAART therapy. Recent Pat CNS Drug Discov antiretroviral treatment: how to sustain success, reduce toxicity
2008; 3:23–33 and ensure adherence avoiding PI use. AIDS 2002; 4:233–241
J Neuropsychiatry Clin Neurosci 22:4, Fall 2010 http://neuro.psychiatryonline.org 367
NEUROPSYCHIATRIC COMPLICATIONS OF EFAVIRENZ THERAPY
7. Cespedes MS, Aberg JA: Neuropsychiatric complications of 26. US Department of Health and Human Services: AIDSinfo.
antiretroviral therapy. Drug Saf 2006; 29:865– 874 Available at http://www.aidsinfo.nih.gov/
8. World Health Organization: Efavirenz 200 mg Capsules (Ran- 27. Blanch J, Martı́nez E, Rousaud A, et al: Preliminary data of a
baxy), HA305. 2007. Available at http://apps.who.int/prequal/ prospective study on neuropsychiatric side effects after initi-
WHOPAR/WHOPARPRODUCTS/HA305Part6v1.pdf ation of efavirenz. J Acquir Immune Defic Syndr 2001; 27:336 –
9. Treisman GJ, Kaplin AI: Neurological and psychiatric compli- 343
cations of antiretroviral agents. AIDS 2002; 16:1201–1215 28. Goldenberg D, Boyle B: Psychiatric safety of efavirenz (ab-
10. Allavena C, Le Moal G, Michau C, et al: Neuropsychiatric stract WePeB4238). Durban, South Africa, XIII Conference on
adverse events after switching from an antiretroviral regimen AIDS, 2000. Available at http://gateway.nlm.nih.gov/
containing efavirenz without tenofovir to an efavirenz regi- MeetingAbstracts/ma?f⫽102240450.html
men containing tenofovir: a report of nine cases. Antivir Ther 29. Gill MJ, Rachlis A, Walmsley S, et al: Canadian Expert Panel
2006; 11:263–265 recommendations on the management of CNS symptoms re-
11. Foster R, Olajide D, Everall IP: Antiretroviral therapy-induced lated to efavirenz. Can J Infect Dis 2001; 12:20c–30c
psychosis: case report and brief review of the literature. HIV 30. Halman M: Management of depression associated with HIV/
Med 2003; 4:139 –144 AIDS and antiretroviral therapy. Can J Infect Dis Med Micro-
12. de la Garza CL, Paoletti-Duarte S, Garcı́a-Martı́n C, et al: biol 2006; 17:5D–9D
Efavrienz-induced psychosis. AIDS 2001; 15:1911–1912 31. von Giesen HJ, Köller H, de Nocker D, et al: Long-term safety
13. Moreno A, Labelle C, Samet JH: Recurrence of post-traumatic and efficacy of NNRTI within the central nervous system. HIV
stress disorder symptoms after initiation of antiretrovirals in- Clin Trials 2003; 4:382–390
cluding efavirenz: a report of two cases. HIV Med 2003; 4:302– 32. Lochet P, Peyrière H, Lotthé A, et al: Long-term assessment of
304 neuropsychiatric adverse reactions associated with efavirenz.
14. Peyriere H, Mauboussin JM, Rouanet I, et al: Management of HIV Med 2003; 4:62– 66
sudden psychiatric disorders related to efavirenz. AIDS 2001; 33. Clifford DB, Evans S, Yang Y, et al: Impact of efavirenz on
15:1323–1324 neuropsychological performance and symptoms in HIV-in-
15. Puzantian T: Central nervous system adverse effects with efa- fected individuals. Ann Intern Med 2005; 143:714 –721
virenz: case report and review. Pharmacotherapy 2002; 22: 34. Ferrando SJ, Gorp W, McElhiney M, et al: Highly active anti-
930 –933 retroviral treatment (HAART) in HIV infection: benefits for
16. Fumaz CR, Muñoz-Moreno JA, Moltó J, et al: Long-term neu- neuropsychological function. AIDS 1998; 12:F65–F70
ropsychiatric disorders on Efavirenz-based approaches. Clin 35. Ferrando SJ, Rablik JG, Gorp W, et al: Longitudinal improve-
Sci 2005; 38:560 –565 ment in psychomotor processing speed is associated with po-
17. Hawkins T, Geist C, Young B, et al: Comparison of neuropsy- tent combination antiretroviral therapy in HIV-1 infection.
chiatric side effects in an observational cohort of efavirenz- J Neuropsychiatry Clin Neurosci 2003; 15:208 –214
and protease inhibitor-treated patients. HIV Clin Trials 2005; 36. Giesen HJ, Theisen A, Arendt G: Therapeutic effects of non-
6:187–196 nucleoside reverse transcriptase inhibitors on the central ner-
18. Rihs TA, Begley K, Smith DE, et al: Efavirenz and chronic vous system in HIV-1-infected patients. J Acquir Immune
neuropsychiatric symptoms: a cross-sectional case control Defic Syndr 2002; 29:363–367
study. HIV Med 2006; 7:544 –548 37. Sacktor N, Schifitto G, McDermott MP, et al: Transdermal
19. Pérez-Molina JA: Safety and tolerance of efavirenz in different selegiline in HIV-associated cognitive impairment: pilot, pla-
antiretroviral regimens: results from a national multicenter cebo-controlled study. Neurology 2000; 54:233–235
prospective study in 1,033 HIV-infected patients. HIV Clin 38. Ruiz NM, Bessen LJ, Manion DJ: Potential adverse experiences
Trials 2002; 3:279 –286 associated with efavirenz in adults (abstract 655). Chicago, 6th
20. Haas DW, Ribaudo HJ, Kim RB, et al: Pharmacogenetics of Conference on Retroviruses and Opportunistic Infections, 1999.
efavirenz and central nervous system side effects: an adult Available at http://gateway.nlm.nih.gov/MeetingAbstracts/
AIDS clinical trials group study. AIDS 2004; 18:2391–2400 ma?f⫽102195420.html
21. Hasse B, Günthard HF, Bleiber G, et al: Efavirenz intoxication 39. Stuss DT, Alexander MP: Is there a dysexecutive syndrome?
due to slow hepatic metabolism. Clin Infect Dis 2005; 40:22–23 Philos Trans R Soc Lond B Biol Sci 2007; 362:901–915
22. Kappelhoff BS, Leth F, Robinson PA, et al: Are adverse events 40. Baumeister RF, Vohs KD (eds): Handbook of Self-Regulation:
of nevirapine and efavirenz related to plasma concentrations? Research, Theory, and Applications. New York, Guilford, 2004
Antivir Ther 2005; 10:489 – 498 41. Banfield JF, Wyland CL, Macrae CN, et al: The cognitive neu-
23. Lowenhaupt EA, Matson K, Qureishi B, et al: Psychosis in a roscience of self-regulation, in Handbook of Self-Regulation.
12-year-old HIV-positive girl with an increased serum concen- Edited by Baumeister RF, Vohs KD. New York, Guilford, 2004,
tration of efavirenz. Clin Infect Dis 2007; 45:128 –130 pp 62– 83
24. Marzolini C, Telenti A, Decosterd LA, et al: Efavirenz plasma 42. Fassbender C, Murphy K, Foxe J, et al: A topography of ex-
levels can predict treatment failure and central nervous sys- ecutive functions revealed by functional magnetic resonance
tem side effects in HIV-1-infected patients. AIDS 2001; 15: imaging. Cogn Brain Res 2004; 20:132–143
71–75 43. Salmon E, Collette F: Functional imaging of executive func-
25. Rotger M, Colombo S, Furrer H, et al: Influence of CYP2B6 tions. Acta Neurol Belg 2005; 105:187–196
polymorphism on plasma and intracellular concentrations 44. Thayer JF, Brosschot JF: Psychosomatics and psychopathol-
and toxicity of efavirenz and nevirapine in HIV-infected pa- ogy: looking up and down from the brain. Psychoneuroendo-
tients. Pharmacogenet Genomics 2005; 15:1–5 crinology 2005; 30:1050 –1058
368 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 22:4, Fall 2010
SÜTTERLIN et al.
45. Thayer JF, Lane RD: A model of neurovisceral integration in 55. Sumich AL, Kumari V, Heasman BC, et al: Abnormal asym-
emotion regulation and dysregulation. J Affect Disord 2000; metry of N200 and P300 event-related potentials in subclinical
61:201–216 depression. J Affect Disord 2006; 92:171–183
46. Knoch D, Fehr E: Resisting the power of temptations: the right 56. Konishi S, Nakajima K, Idai U, et al: Transient activation of
prefrontal cortex and self-control. Ann N Y Acad Sci 2007; inferior prefrontal cortex during cognitive set shifting. Nat
1104:123–134 Neurosci 1998; 1:80 – 84
47. Segerstrom SC, Solberg Nes L: Heart rate variability reflects 57. Konishi S, Kyoichi N, Idai U, et al: Common inhibitory mech-
self-regulatory strength, effort, and fatigue. Psychol Sci 2007;
anism in human inferior prefrontal cortex revealed by event-
18:275–281
related functional MRI. Brain 1999; 122:981–991
48. Siepmann M, Aykac V, Unterdörfer J, et al: A pilot study on
58. Chamberlain SR, Sahakian BJ: The neuropsychiatry of impul-
the effects of heart rate variability biofeedback in patients with
depression and in healthy subjects. Appl Psychophysiol sivity. Curr Opin Psychiatry 2007; 20:255–261
Biofeedback 2008; 33:195–201 59. Gorman JM, Sloan RP: Heart rate variability in depressive and
49. Reiner R: Integrating a portable biofeedback device into clin- anxiety disorders. Am Heart J 2000; 140:77– 83
ical practice for patients with anxiety disorders: results of a 60. Friedman BH: An autonomic flexibility-neurovisceral integra-
pilot study. Appl Psychophysiol Biofeedback 2008; 33:55– 61 tion model of anxiety and cardiac vagal tone. Biol Psychol
50. Colcombe SJ, Kramer AF, Erickson KI, et al: Cardiovascular 2007; 74:185–199
fitness, cortical plasticity, and aging. Proc Natl Acad Sci U S A 61. Thayer JF, Lane RD: Claude Bernard and the heart-brain con-
2004; 101:3316 –3321 nection: further elaboration of a model of neurovisceral inte-
51. Hansen AL, Johnsen BH, Sollers JJ, et al: Heart rate variability gration. Neurosci Biobehav Rev 2009; 33:81–88
and its relation to prefrontal cognitive function: the effects of 62. Thayer JF, Hansen AL, Saus-Rose E, et al: Heart rate vari-
training and detraining. Eur J Applied Physiology 2004; 93: ability, prefrontal neural function, and cognitive perfor-
263–272 mance: the neurovisceral integration perspective on self-
52. Kawashima R, Sato K, Itoh H, et al: Functional anatomy of
regulation, adaptation, and health. Ann Behav Med 2009;
GO/NO-GO discrimination and response selection: a PET
37:141–153
study in man. Brain Res 1996; 728:79 – 89
63. Barkley R: The executive functions and self-regulation: an
53. Zheng D, Oka T, Bokura H, et al: The key locus of common
response inhibition network for no-go and stop-signals. J evolutionary neuropsychological perspective. Neuropsycho-
Cogn Neurosci 2008; 20:1434 –1442 logical Rev 2001; 11:1–29
54. Patel SH, Azzam PN: Characterization of N200 and P300: 64. Miyake A, Emerson MJ, Friedman NP: Assessment of execu-
selected studies of the event-related potential. Int J Med Sci tive functions in clinical settings: problems and recommenda-
2005; 2:147–154 tions. Semin Speech Lang 2000; 21:169 –183
J Neuropsychiatry Clin Neurosci 22:4, Fall 2010 http://neuro.psychiatryonline.org 369
Vous aimerez peut-être aussi
- SULPYCO Method: A New Quantum and Integrative Approach to DepressionD'EverandSULPYCO Method: A New Quantum and Integrative Approach to DepressionPas encore d'évaluation
- Kenedi 2011Document16 pagesKenedi 2011IAPas encore d'évaluation
- J 1600-0447 2006 00787 XDocument11 pagesJ 1600-0447 2006 00787 XAnonymous hyUqzpSPas encore d'évaluation
- Psychotic Disorders Induced by Antiepileptic Drugs in People With EpilepsyDocument11 pagesPsychotic Disorders Induced by Antiepileptic Drugs in People With EpilepsydupuytrenPas encore d'évaluation
- WangDocument9 pagesWangIolanda PălimaruPas encore d'évaluation
- Tolchin2020 Neurop. Epilepsia 2020Document16 pagesTolchin2020 Neurop. Epilepsia 2020Carolina MuñozPas encore d'évaluation
- Eschizophrenia ResearchDocument8 pagesEschizophrenia ResearchZoila ChávezPas encore d'évaluation
- The Association Between Anomalous Self-E PDFDocument5 pagesThe Association Between Anomalous Self-E PDFferny zabatierraPas encore d'évaluation
- Epilepsy & Behavior: Ali A. Asadi-Pooya, Jennifer TinkerDocument3 pagesEpilepsy & Behavior: Ali A. Asadi-Pooya, Jennifer TinkerNico NicoPas encore d'évaluation
- Adherence With Psychotherapy and Treatment Outcomes With Psychogenic Nonepileptic SeizuresDocument6 pagesAdherence With Psychotherapy and Treatment Outcomes With Psychogenic Nonepileptic SeizuresNely M. RosyidiPas encore d'évaluation
- A Qualitative Research Case StudyDocument3 pagesA Qualitative Research Case StudyAndrea AtonducanPas encore d'évaluation
- Treat AcuteDocument8 pagesTreat AcuteShane LeePas encore d'évaluation
- Patterns and Frequency of Atypical Antipsychotic Prescribing in Psychiatric Medical Centers: A Cross-Sectional National SurveyDocument9 pagesPatterns and Frequency of Atypical Antipsychotic Prescribing in Psychiatric Medical Centers: A Cross-Sectional National Surveymiron_ghiuPas encore d'évaluation
- Sesgos de Memoria en Los Trastornos de AnsiedadDocument15 pagesSesgos de Memoria en Los Trastornos de AnsiedadIMHPas encore d'évaluation
- Psychotic Disorders Induced by Antiepileptic Drugs in People With EpilepsyDocument11 pagesPsychotic Disorders Induced by Antiepileptic Drugs in People With EpilepsyDr. Jonathan CampilloPas encore d'évaluation
- Management of Insomnia and Anxiety in Myasthenia GravisDocument6 pagesManagement of Insomnia and Anxiety in Myasthenia Gravisilmiah neurologiPas encore d'évaluation
- JPR 15 2211Document11 pagesJPR 15 2211natneednutPas encore d'évaluation
- Pi Is 0025712514000893Document32 pagesPi Is 0025712514000893Christoph HockPas encore d'évaluation
- Mixed AnxietyDocument2 pagesMixed Anxietyarif rhPas encore d'évaluation
- Anxiety and Mood Disorders in Narcolepsy: A Case - Control StudyDocument8 pagesAnxiety and Mood Disorders in Narcolepsy: A Case - Control StudyDesyifa Annisa MursalinPas encore d'évaluation
- Obsessive Compulsivedisorder (OCD) PracticalstrategiesDocument12 pagesObsessive Compulsivedisorder (OCD) PracticalstrategiesAF KoasPas encore d'évaluation
- Can Long-Term Treatment With Antidepressant Drugs Worsen The Course of Depression?Document11 pagesCan Long-Term Treatment With Antidepressant Drugs Worsen The Course of Depression?Ziggy GonPas encore d'évaluation
- Admin, ZIK LECTURE JOURNAL-82-91Document10 pagesAdmin, ZIK LECTURE JOURNAL-82-91ElenaPas encore d'évaluation
- Seizure: European Journal of Epilepsy: SciencedirectDocument7 pagesSeizure: European Journal of Epilepsy: SciencedirectMaria Von ShaftPas encore d'évaluation
- Antipsychotic Polypharmacy For The Management of SchizophreniaDocument12 pagesAntipsychotic Polypharmacy For The Management of SchizophreniaAlondra CastilloPas encore d'évaluation
- Novakova 2015Document7 pagesNovakova 2015esckere papas fritasPas encore d'évaluation
- WFSBP Treatment Guidelines Dementia PDFDocument31 pagesWFSBP Treatment Guidelines Dementia PDFALLPas encore d'évaluation
- Nonepileptic Seizures - An Updated ReviewDocument9 pagesNonepileptic Seizures - An Updated ReviewCecilia FRPas encore d'évaluation
- Generalized Anxiety DisorderDocument8 pagesGeneralized Anxiety DisorderTanvi SharmaPas encore d'évaluation
- NDT 81677 Adherence and Re Hospitalizations in Patients With Schizophr 040115Document6 pagesNDT 81677 Adherence and Re Hospitalizations in Patients With Schizophr 040115Elsa OctaviaPas encore d'évaluation
- Psychogenic Nonepileptic Seizures - Management and Prognosis - UpToDateDocument18 pagesPsychogenic Nonepileptic Seizures - Management and Prognosis - UpToDateAndré MendonçaPas encore d'évaluation
- Artigo NFD Efficacy of Invasive and Non-Invasive Brain ModulationDocument23 pagesArtigo NFD Efficacy of Invasive and Non-Invasive Brain ModulationMarcelo MenezesPas encore d'évaluation
- Prescribing Antipsychotics in Geriatric Patients:: First of 3 PartsDocument8 pagesPrescribing Antipsychotics in Geriatric Patients:: First of 3 PartsAlexRázuri100% (1)
- 2021, EPA - Guidance - On - Treatment - of - NDocument16 pages2021, EPA - Guidance - On - Treatment - of - Nfelix08121992Pas encore d'évaluation
- Psychopharmacological Treatment of Obsessive-Compulsive Disorder (OCD)Document27 pagesPsychopharmacological Treatment of Obsessive-Compulsive Disorder (OCD)godolfintorentPas encore d'évaluation
- Silexan in Anxiety Disorders: Clinical Data and Pharmacological BackgroundDocument10 pagesSilexan in Anxiety Disorders: Clinical Data and Pharmacological BackgroundCanal da Bia E do GutoPas encore d'évaluation
- Effect of Anxiety Disorder On Impairment and Recovery From StrokeDocument7 pagesEffect of Anxiety Disorder On Impairment and Recovery From StrokeRatnaWFebryPas encore d'évaluation
- Disosiatif KonversiDocument14 pagesDisosiatif KonversiArv IraPas encore d'évaluation
- PsychologyDocument7 pagesPsychologyHarish KumarPas encore d'évaluation
- Title: Prevalence and Factors Associated With Extrapyramidal Side Effects Among Inpatients at A Tertiary Care Setting: A Cross-Sectional StudyDocument7 pagesTitle: Prevalence and Factors Associated With Extrapyramidal Side Effects Among Inpatients at A Tertiary Care Setting: A Cross-Sectional StudyAbdul Mannan ChatthaPas encore d'évaluation
- Pharmacotherapy of Anxiety Disorders - A Critical ReviewDocument15 pagesPharmacotherapy of Anxiety Disorders - A Critical Reviewsruso1Pas encore d'évaluation
- PNES ClinicalApproachesDocument19 pagesPNES ClinicalApproachesClaudiaPas encore d'évaluation
- Add-On Pharmacotherapy For PatientsDocument2 pagesAdd-On Pharmacotherapy For PatientsmarcoPas encore d'évaluation
- Psychogenic Non-Epileptic Seizures A Narrative Review: Archives of Academic Emergency Medicine. 2020 8 (1) : E10Document7 pagesPsychogenic Non-Epileptic Seizures A Narrative Review: Archives of Academic Emergency Medicine. 2020 8 (1) : E10Axel Robinson HerreraPas encore d'évaluation
- Research PaperDocument8 pagesResearch Paperapi-698797022Pas encore d'évaluation
- A Randomized Controlled Trial of A Mindfulness-Based Intervention Program For People With Schizophrenia: 6-Month Follow-UpDocument14 pagesA Randomized Controlled Trial of A Mindfulness-Based Intervention Program For People With Schizophrenia: 6-Month Follow-UpOrion OriPas encore d'évaluation
- Psychobiology Schizophrenia Research Paper FINAL (At)Document8 pagesPsychobiology Schizophrenia Research Paper FINAL (At)gucci manePas encore d'évaluation
- Anxiety, Mood, and Personality Disorders in Patients With Benign Paroxysmal Positional VertigoDocument5 pagesAnxiety, Mood, and Personality Disorders in Patients With Benign Paroxysmal Positional VertigoOkim NawarPas encore d'évaluation
- 2017-Psychological Interventions For Psychogenic Non Epileptic SeizuresDocument9 pages2017-Psychological Interventions For Psychogenic Non Epileptic SeizuresFidel ArroyoPas encore d'évaluation
- Antidepressants For The Treatment of NarcolepsyDocument5 pagesAntidepressants For The Treatment of NarcolepsyMOHAMAD FAKIHPas encore d'évaluation
- Psicofármacos y VIHDocument8 pagesPsicofármacos y VIHANDREA MATAMOROSPas encore d'évaluation
- SCHIZOPHRENIFORMDocument5 pagesSCHIZOPHRENIFORMThrift AdvisoryPas encore d'évaluation
- Chronic Insomnia: Matt T. Bianchi, MD, PHDDocument6 pagesChronic Insomnia: Matt T. Bianchi, MD, PHDAlex BorroelPas encore d'évaluation
- Depresión Psicotica 2024 LancetDocument11 pagesDepresión Psicotica 2024 LancetJuan ParedesPas encore d'évaluation
- Sniffing Around Oxytocin: Review and Meta-Analyses of Trials in Healthy and Clinical Groups With Implications For PharmacotherapyDocument15 pagesSniffing Around Oxytocin: Review and Meta-Analyses of Trials in Healthy and Clinical Groups With Implications For PharmacotherapyVanilla BakePas encore d'évaluation
- 1 s2.0 S2173580821000432 Main PDFDocument10 pages1 s2.0 S2173580821000432 Main PDFAFlor DuranPas encore d'évaluation
- E Cacy of Modern Antipsychotics in Placebo-Controlled Trials in Bipolar Depression: A Meta-AnalysisDocument10 pagesE Cacy of Modern Antipsychotics in Placebo-Controlled Trials in Bipolar Depression: A Meta-AnalysisRisda AprilianiPas encore d'évaluation
- Reviewing Depot Injection Efficacy in The Treatment of SchizophreniaDocument10 pagesReviewing Depot Injection Efficacy in The Treatment of SchizophreniaAnonymous raLgWVyqPas encore d'évaluation
- What We Know and What We Don't Know About The Treatment of Schizoaffective DisorderDocument11 pagesWhat We Know and What We Don't Know About The Treatment of Schizoaffective DisorderAshPas encore d'évaluation
- Off-Label Use of Sodium Valproate For SchizophreniaDocument7 pagesOff-Label Use of Sodium Valproate For SchizophreniaHaya GrinvaldPas encore d'évaluation
- tmpEFCC TMPDocument6 pagestmpEFCC TMPFrontiersPas encore d'évaluation
- tmpCE8C TMPDocument19 pagestmpCE8C TMPFrontiersPas encore d'évaluation
- tmp3CAB TMPDocument16 pagestmp3CAB TMPFrontiersPas encore d'évaluation
- tmp80F6 TMPDocument24 pagestmp80F6 TMPFrontiersPas encore d'évaluation
- tmpF178 TMPDocument15 pagestmpF178 TMPFrontiersPas encore d'évaluation
- Tmp1a96 TMPDocument80 pagesTmp1a96 TMPFrontiersPas encore d'évaluation
- tmp6F0E TMPDocument12 pagestmp6F0E TMPFrontiersPas encore d'évaluation
- tmp72FE TMPDocument8 pagestmp72FE TMPFrontiersPas encore d'évaluation
- tmp37B8 TMPDocument9 pagestmp37B8 TMPFrontiersPas encore d'évaluation
- Tmpa077 TMPDocument15 pagesTmpa077 TMPFrontiersPas encore d'évaluation
- tmpE7E9 TMPDocument14 pagestmpE7E9 TMPFrontiersPas encore d'évaluation
- tmpF3B5 TMPDocument15 pagestmpF3B5 TMPFrontiersPas encore d'évaluation
- tmpFFE0 TMPDocument6 pagestmpFFE0 TMPFrontiersPas encore d'évaluation
- tmpE3C0 TMPDocument17 pagestmpE3C0 TMPFrontiersPas encore d'évaluation
- tmpF407 TMPDocument17 pagestmpF407 TMPFrontiersPas encore d'évaluation
- tmp60EF TMPDocument20 pagestmp60EF TMPFrontiersPas encore d'évaluation
- tmp6382 TMPDocument8 pagestmp6382 TMPFrontiersPas encore d'évaluation
- tmp998 TMPDocument9 pagestmp998 TMPFrontiersPas encore d'évaluation
- tmpC0A TMPDocument9 pagestmpC0A TMPFrontiersPas encore d'évaluation
- tmpA0D TMPDocument9 pagestmpA0D TMPFrontiersPas encore d'évaluation
- tmp4B57 TMPDocument9 pagestmp4B57 TMPFrontiersPas encore d'évaluation
- tmp8B94 TMPDocument9 pagestmp8B94 TMPFrontiersPas encore d'évaluation
- tmpD1FE TMPDocument6 pagestmpD1FE TMPFrontiersPas encore d'évaluation
- tmp27C1 TMPDocument5 pagestmp27C1 TMPFrontiersPas encore d'évaluation
- tmp2F3F TMPDocument10 pagestmp2F3F TMPFrontiersPas encore d'évaluation
- tmpB1BE TMPDocument9 pagestmpB1BE TMPFrontiersPas encore d'évaluation
- tmp9D75 TMPDocument9 pagestmp9D75 TMPFrontiersPas encore d'évaluation
- Tmp75a7 TMPDocument8 pagesTmp75a7 TMPFrontiersPas encore d'évaluation
- tmpC30A TMPDocument10 pagestmpC30A TMPFrontiersPas encore d'évaluation
- tmp3656 TMPDocument14 pagestmp3656 TMPFrontiersPas encore d'évaluation
- Propuesta de Un Protocolo para La Evaluación de Las Funciones EjecutivasDocument10 pagesPropuesta de Un Protocolo para La Evaluación de Las Funciones EjecutivasIsaura Calderón M.Pas encore d'évaluation
- Multitasking Science FairDocument21 pagesMultitasking Science FairJenna vdnPas encore d'évaluation
- Adele DiamondsDocument5 pagesAdele Diamondsgina1975Pas encore d'évaluation
- Positive Intelligence Webinar (Handout)Document26 pagesPositive Intelligence Webinar (Handout)Spil_vv_IJmuiden100% (3)
- DPNDocument7 pagesDPNFikry SyahrialPas encore d'évaluation
- NICABM BruceLipton Brain2014Document34 pagesNICABM BruceLipton Brain2014acehussainPas encore d'évaluation
- Primitive Brain Is 'Smarter' Than We Think, MIT Study Shows - ScienceDaily PDFDocument2 pagesPrimitive Brain Is 'Smarter' Than We Think, MIT Study Shows - ScienceDaily PDFAnonymous TwMqdTP8G4Pas encore d'évaluation
- Phineas Gage Story and Questions - Abeni HarrisDocument4 pagesPhineas Gage Story and Questions - Abeni HarrisAbeni HarrisPas encore d'évaluation
- Beyond Emotional IntelligenceDocument190 pagesBeyond Emotional Intelligencecipioo7Pas encore d'évaluation
- Iveyand DanielsDocument22 pagesIveyand DanielsJuan C. VargasPas encore d'évaluation
- Assignment For 29.04.2021Document20 pagesAssignment For 29.04.2021RADHIKA JAISWALPas encore d'évaluation
- Dynamic Child 1st Edition Manis Test Bank DownloadDocument85 pagesDynamic Child 1st Edition Manis Test Bank DownloadChristina Jackson100% (22)
- Report Study Into The Mental Resilience of Journalists DR Tara SwartDocument12 pagesReport Study Into The Mental Resilience of Journalists DR Tara SwartfinntheceltPas encore d'évaluation
- Lewis & Todd, 2007. Self-Regulation Brain PDFDocument25 pagesLewis & Todd, 2007. Self-Regulation Brain PDFStephanie HernándezPas encore d'évaluation
- Psychology: General, 132, 47-70.: Michael J. KaneDocument35 pagesPsychology: General, 132, 47-70.: Michael J. KaneRodolfo Esteban Muñoz GómezPas encore d'évaluation
- EIUS Case Study-1Document5 pagesEIUS Case Study-1Nishan ShettyPas encore d'évaluation
- Expressive Therapy With Traumatized Children by P. Gussie Klorer PDFDocument228 pagesExpressive Therapy With Traumatized Children by P. Gussie Klorer PDFAnca NicoliPas encore d'évaluation
- Perspectives On Psychological Science 2011 Holzel PDFDocument23 pagesPerspectives On Psychological Science 2011 Holzel PDFaranda_88Pas encore d'évaluation
- Bobath Concept - Theory and Clinical Practice in Neurological RehabilitationDocument218 pagesBobath Concept - Theory and Clinical Practice in Neurological Rehabilitationralphholingshead100% (1)
- Learning and Cognitive Flexibility - Frontostriatal Function and Monoaminergic ModulationDocument6 pagesLearning and Cognitive Flexibility - Frontostriatal Function and Monoaminergic ModulationFrancisco Ahumada MéndezPas encore d'évaluation
- AconceptualproposalDocument11 pagesAconceptualproposalVÍCTOR MANUEL NEIRA RUBIOPas encore d'évaluation
- The Psychopath MagnetizedDocument9 pagesThe Psychopath MagnetizedAvengingBrainPas encore d'évaluation
- Emergence of Hyper Empathy After Right ADocument5 pagesEmergence of Hyper Empathy After Right AIngrid HurwitzPas encore d'évaluation
- Complex Imitation and The Language-Ready BrainDocument40 pagesComplex Imitation and The Language-Ready BrainJenny sunPas encore d'évaluation
- First Few Seconds For FlowDocument18 pagesFirst Few Seconds For FlowMateiDCPas encore d'évaluation
- Brain System DR Daniel AmenDocument2 pagesBrain System DR Daniel AmenBharat Shah100% (1)
- The Vulcanization of BrainDocument30 pagesThe Vulcanization of BrainJohnny FragosoPas encore d'évaluation
- Working Memory and The MindDocument8 pagesWorking Memory and The MindAca AvPas encore d'évaluation
- CapstoneessayglaneDocument12 pagesCapstoneessayglaneapi-251768051Pas encore d'évaluation
- The Brain-Changing Benefits of Exercise - Wendy SuzukiDocument5 pagesThe Brain-Changing Benefits of Exercise - Wendy SuzukiAF Ann RossPas encore d'évaluation
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDD'EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDÉvaluation : 4.5 sur 5 étoiles4.5/5 (167)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryD'EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryÉvaluation : 4.5 sur 5 étoiles4.5/5 (157)
- An Autobiography of Trauma: A Healing JourneyD'EverandAn Autobiography of Trauma: A Healing JourneyÉvaluation : 5 sur 5 étoiles5/5 (2)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisD'EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (9)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreD'EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreÉvaluation : 5 sur 5 étoiles5/5 (17)
- The Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItD'EverandThe Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (107)
- Don't Panic: Taking Control of Anxiety AttacksD'EverandDon't Panic: Taking Control of Anxiety AttacksÉvaluation : 4 sur 5 étoiles4/5 (12)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeD'EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeÉvaluation : 4.5 sur 5 étoiles4.5/5 (140)
- Redefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackD'EverandRedefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackÉvaluation : 4.5 sur 5 étoiles4.5/5 (152)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeD'EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeÉvaluation : 4.5 sur 5 étoiles4.5/5 (49)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionD'EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionPas encore d'évaluation
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsD'EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsÉvaluation : 4.5 sur 5 étoiles4.5/5 (39)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisD'EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisÉvaluation : 5 sur 5 étoiles5/5 (5)
- A Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentD'EverandA Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentPas encore d'évaluation
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeD'EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeÉvaluation : 5 sur 5 étoiles5/5 (559)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesD'EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesÉvaluation : 5 sur 5 étoiles5/5 (70)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveD'EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveÉvaluation : 4 sur 5 étoiles4/5 (250)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaD'EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (56)
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationD'EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationÉvaluation : 5 sur 5 étoiles5/5 (9)
- How to Be Miserable: 40 Strategies You Already UseD'EverandHow to Be Miserable: 40 Strategies You Already UseÉvaluation : 4.5 sur 5 étoiles4.5/5 (57)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouD'EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouPas encore d'évaluation
- The Anatomy of Loneliness: How to Find Your Way Back to ConnectionD'EverandThe Anatomy of Loneliness: How to Find Your Way Back to ConnectionÉvaluation : 4.5 sur 5 étoiles4.5/5 (162)
- 50 Ways to Rewire Your Anxious Brain: Simple Skills to Soothe Anxiety and Create New Neural Pathways to CalmD'Everand50 Ways to Rewire Your Anxious Brain: Simple Skills to Soothe Anxiety and Create New Neural Pathways to CalmPas encore d'évaluation
- The Popular Encyclopedia of Christian Counseling: An Indispensable Tool for Helping People with Their ProblemsD'EverandThe Popular Encyclopedia of Christian Counseling: An Indispensable Tool for Helping People with Their ProblemsÉvaluation : 5 sur 5 étoiles5/5 (1)