Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Introduction To BioethicsDocument33 pagesIntroduction To BioethicsReymart BolagaoPas encore d'évaluation
- AA Course-Difficult Airway1Document54 pagesAA Course-Difficult Airway1Anonymous V5xDcrPas encore d'évaluation
- AJACM 2010 5 2 Wang Juyi Interview Part 1 of 2 - LiuDocument7 pagesAJACM 2010 5 2 Wang Juyi Interview Part 1 of 2 - LiuYagtaliPas encore d'évaluation
- 000-Intro To Internal MedicineDocument6 pages000-Intro To Internal MedicineRizky KykyPas encore d'évaluation
- Cancer Goes Viral: HPV-positive Throat and Tongue Cancers Are Taking Off in MenDocument2 pagesCancer Goes Viral: HPV-positive Throat and Tongue Cancers Are Taking Off in MenMEGA_ONEPas encore d'évaluation
- Trade/Generic Name Classification Action of Medication Dosage/Route/ Frequency Indications For Use (Patient Specific)Document16 pagesTrade/Generic Name Classification Action of Medication Dosage/Route/ Frequency Indications For Use (Patient Specific)lightzapPas encore d'évaluation
- BFSA-Volume 46-Issue 1 - Page 647-657Document11 pagesBFSA-Volume 46-Issue 1 - Page 647-657mizranitaPas encore d'évaluation
- Name: Aisyah Amalyah Putri NIM: 21114030Document2 pagesName: Aisyah Amalyah Putri NIM: 21114030Dedikaka CoyPas encore d'évaluation
- BPUDDocument26 pagesBPUDIvanPas encore d'évaluation
- Laporan Bulanan Lb1: 0-7 HR Baru LDocument20 pagesLaporan Bulanan Lb1: 0-7 HR Baru LOla SarlinaPas encore d'évaluation
- PeritonitisDocument21 pagesPeritonitischrisyenPas encore d'évaluation
- Vit KDocument2 pagesVit KBilly Jeremia TandoPas encore d'évaluation
- Professional PhilosophyDocument8 pagesProfessional Philosophyapi-450228862Pas encore d'évaluation
- PGIMER Chandigarh Recruitment 2022 Notification Group A B C PostsDocument36 pagesPGIMER Chandigarh Recruitment 2022 Notification Group A B C PostsGourav KadianPas encore d'évaluation
- Worksheet 8Document2 pagesWorksheet 8Jocel OclaritPas encore d'évaluation
- of M.pharmDocument13 pagesof M.pharmVivek Patel ViksPas encore d'évaluation
- Uporaba Metoda Palijativne Skrbi U Djece Implementation of Palliative Care Methods in ChildrenDocument7 pagesUporaba Metoda Palijativne Skrbi U Djece Implementation of Palliative Care Methods in ChildrenMoonyPas encore d'évaluation
- Understanding PhlebotomyDocument4 pagesUnderstanding PhlebotomyAngelo Jude CumpioPas encore d'évaluation
- Draw-Over Anaesthesia - DobsonDocument7 pagesDraw-Over Anaesthesia - DobsonHuynh Quoc SangPas encore d'évaluation
- Tonetti Et Al-2018-Journal of Periodontology TDocument14 pagesTonetti Et Al-2018-Journal of Periodontology TJonathan Meza MauricioPas encore d'évaluation
- Oral Lichen PlanusDocument28 pagesOral Lichen PlanusParul SinghPas encore d'évaluation
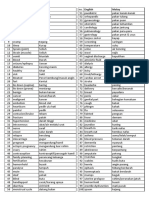
- Medic Term English MalayDocument1 pageMedic Term English MalaySyamimi SuhaimiPas encore d'évaluation
- 3365460Document3 pages3365460Mohamed NabilPas encore d'évaluation
- Intubation - Gastrointestinal TractDocument2 pagesIntubation - Gastrointestinal TractDominion OgochukwuPas encore d'évaluation
- Cebu Declaration List of ParticipantsDocument6 pagesCebu Declaration List of ParticipantspuspaPas encore d'évaluation
- Scars Healing 5 11Document4 pagesScars Healing 5 11Nishant NeogyPas encore d'évaluation
- Parasagittal MeningiomaDocument51 pagesParasagittal MeningiomaAji Setia UtamaPas encore d'évaluation
- Case 4Document5 pagesCase 4angelica dizonPas encore d'évaluation
- Pemicu 6 Blok Saraf Dan KejiwaanDocument44 pagesPemicu 6 Blok Saraf Dan KejiwaanTommy WidjajaPas encore d'évaluation
- Cover Letter Heidi BosmansDocument1 pageCover Letter Heidi Bosmansapi-283672381Pas encore d'évaluation