Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- DNV Os C104 2014Document40 pagesDNV Os C104 2014Moe LattPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Physics For Entertainment Volume 1 (Yakov Perelman)Document211 pagesPhysics For Entertainment Volume 1 (Yakov Perelman)snath7800Pas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Final EstimateDocument60 pagesFinal EstimateChristian Paulo Cardinal TungolPas encore d'évaluation
- A Singer's Notes: Preventing Vocal Nodules: Teresa Radomski, MMDocument21 pagesA Singer's Notes: Preventing Vocal Nodules: Teresa Radomski, MMDanis WaraPas encore d'évaluation
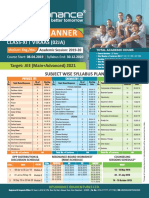
- Reso Course PlannerDocument2 pagesReso Course PlannerSnehasishGhosh100% (1)
- Turbo Expander TrainingDocument58 pagesTurbo Expander TrainingM Joko Susilo100% (6)
- High Performance Techniques For Microsoft SQL Server PDFDocument307 pagesHigh Performance Techniques For Microsoft SQL Server PDFmaghnus100% (1)
- (Advances in Cryogenic Engineering 37) Takayuki Kishi, Mizuo Kudo, Hiromasa Iisaka (Auth.), R. W. Fast (Eds.) - Advances in Cryogenic Engineering-Springer US (1991)Document729 pages(Advances in Cryogenic Engineering 37) Takayuki Kishi, Mizuo Kudo, Hiromasa Iisaka (Auth.), R. W. Fast (Eds.) - Advances in Cryogenic Engineering-Springer US (1991)ksvvijPas encore d'évaluation
- Blockchain Unconfirmed Transaction Hack Script Docx PDF FreeDocument2 pagesBlockchain Unconfirmed Transaction Hack Script Docx PDF FreeHealing Relaxing Sleep Music100% (1)
- Mos RamDocument15 pagesMos RamDr. MNV KiranbabuPas encore d'évaluation
- Derajat Paresis Nervus FasialisDocument1 pageDerajat Paresis Nervus FasialisDiah HayustiningsihPas encore d'évaluation
- Journal BBLRDocument17 pagesJournal BBLRDiah HayustiningsihPas encore d'évaluation
- Derajat Paresis Nervus FasialisDocument1 pageDerajat Paresis Nervus FasialisDiah HayustiningsihPas encore d'évaluation
- 2010 Article 116Document6 pages2010 Article 116Diah HayustiningsihPas encore d'évaluation
- 149 157 PDFDocument9 pages149 157 PDFDiah HayustiningsihPas encore d'évaluation
- Journal BBLRDocument17 pagesJournal BBLRDiah HayustiningsihPas encore d'évaluation
- 149 157 PDFDocument9 pages149 157 PDFDiah HayustiningsihPas encore d'évaluation
- 2011 Article 271Document4 pages2011 Article 271Diah HayustiningsihPas encore d'évaluation
- Intervensi Rehabilitasi RHSDocument6 pagesIntervensi Rehabilitasi RHSDiah HayustiningsihPas encore d'évaluation
- Etiologi Conductive Hearing LossDocument12 pagesEtiologi Conductive Hearing LossDiah HayustiningsihPas encore d'évaluation
- 2010 Article 43Document6 pages2010 Article 43Diah HayustiningsihPas encore d'évaluation
- Full Recovery of A 13-Year-Old Boy With Pediatric Ramsay Hunt Syndrome Using A Shorter Course of Aciclovir and Steroid at Lower Doses: A Case ReportDocument4 pagesFull Recovery of A 13-Year-Old Boy With Pediatric Ramsay Hunt Syndrome Using A Shorter Course of Aciclovir and Steroid at Lower Doses: A Case ReportDiah HayustiningsihPas encore d'évaluation
- Tympanometry in Clinical Practice: Janet Shanks and Jack ShohetDocument32 pagesTympanometry in Clinical Practice: Janet Shanks and Jack ShohetDiah HayustiningsihPas encore d'évaluation
- Etiologi Conductive Hearing LossDocument12 pagesEtiologi Conductive Hearing LossDiah HayustiningsihPas encore d'évaluation
- Etiologi Conductive Hearing LossDocument12 pagesEtiologi Conductive Hearing LossDiah HayustiningsihPas encore d'évaluation
- Management of Extensive Dentigerous CystsDocument4 pagesManagement of Extensive Dentigerous CystsAnupama NagrajPas encore d'évaluation
- Steroid Pada RSS CaseDocument3 pagesSteroid Pada RSS CaseDiah HayustiningsihPas encore d'évaluation
- Steroid Pada RSS CaseDocument3 pagesSteroid Pada RSS CaseDiah HayustiningsihPas encore d'évaluation
- O To SclerosisDocument4 pagesO To SclerosisDiah HayustiningsihPas encore d'évaluation
- Steroid Pada RSS CaseDocument3 pagesSteroid Pada RSS CaseDiah HayustiningsihPas encore d'évaluation
- Prognosis RHSDocument6 pagesPrognosis RHSDiah HayustiningsihPas encore d'évaluation
- Muscarella L AJIC 2007 LaryngosDocument9 pagesMuscarella L AJIC 2007 LaryngosDiah HayustiningsihPas encore d'évaluation
- Intervensi Rehabilitasi RHSDocument6 pagesIntervensi Rehabilitasi RHSDiah HayustiningsihPas encore d'évaluation
- Cherub Is MeDocument8 pagesCherub Is MeDiah HayustiningsihPas encore d'évaluation
- Contact Endoscopy As A Novel TechniqueDocument6 pagesContact Endoscopy As A Novel TechniqueDiah HayustiningsihPas encore d'évaluation
- A Prospective Randomized Equivalence Trial of The.21-1Document7 pagesA Prospective Randomized Equivalence Trial of The.21-1Diah HayustiningsihPas encore d'évaluation
- Characteristics and Prognosis of Malignant ExternalDocument3 pagesCharacteristics and Prognosis of Malignant ExternalDiah HayustiningsihPas encore d'évaluation
- Tympanometry in Clinical Practice: Janet Shanks and Jack ShohetDocument32 pagesTympanometry in Clinical Practice: Janet Shanks and Jack ShohetDiah HayustiningsihPas encore d'évaluation
- 1.necrotizing (Malignant) External OtitisDocument4 pages1.necrotizing (Malignant) External OtitisDiah HayustiningsihPas encore d'évaluation
- ES Q2 Mod8Document26 pagesES Q2 Mod8maacovsPas encore d'évaluation
- Bandura Et Al.Document16 pagesBandura Et Al.Siddhant JhawarPas encore d'évaluation
- To Design and Simulate Priority EncoderDocument6 pagesTo Design and Simulate Priority EncoderShubham GargPas encore d'évaluation
- Integumentary SystemDocument8 pagesIntegumentary SystemAshley Brithanie RamosPas encore d'évaluation
- Power Max India PVT LTD Extra Work Done at VMW Shed WorksDocument4 pagesPower Max India PVT LTD Extra Work Done at VMW Shed WorksparthaPas encore d'évaluation
- Nms5Lx 6.6.1: User ManualDocument590 pagesNms5Lx 6.6.1: User ManualGentjan ZogaPas encore d'évaluation
- Install and Configure Computer SystemsDocument18 pagesInstall and Configure Computer SystemsAlbino LarozaPas encore d'évaluation
- Synopsis: in Order To Decrease Cross Sectional Area of Structural Members, Ultra High StrengthDocument16 pagesSynopsis: in Order To Decrease Cross Sectional Area of Structural Members, Ultra High StrengthHector Alberto Garcia LopezPas encore d'évaluation
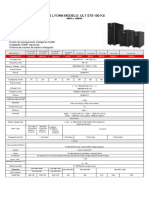
- Ups Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVADocument1 pageUps Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVASebastian Matias CruzPas encore d'évaluation
- Lecture 10 - Dry Etching PDFDocument7 pagesLecture 10 - Dry Etching PDFSiddhant ModiPas encore d'évaluation
- Module 3 - Data and Database ManagementDocument11 pagesModule 3 - Data and Database ManagementDarrilyn VillalunaPas encore d'évaluation
- Technical Guide R-410A ZJ/ZR/ZF Series 15 - 25 TON 60 Hertz: DescriptionDocument103 pagesTechnical Guide R-410A ZJ/ZR/ZF Series 15 - 25 TON 60 Hertz: DescriptionmanthoexPas encore d'évaluation
- Problem 13.3Document2 pagesProblem 13.3kannyPas encore d'évaluation
- Zebralette User GuideDocument24 pagesZebralette User GuideGiacomo TimbrelloPas encore d'évaluation
- Surge Current Protection Using SuperconductorDocument25 pagesSurge Current Protection Using SuperconductorAbhishek Walter PaulPas encore d'évaluation
- H-I SUPER-DEHYDRATION WITH GLYCOLSDocument15 pagesH-I SUPER-DEHYDRATION WITH GLYCOLSDiego1980bPas encore d'évaluation
- B1698Document23 pagesB1698Esteban OrtegaPas encore d'évaluation
- Pages 296-298 Module 6 ReviewDocument4 pagesPages 296-298 Module 6 Reviewapi-332361871Pas encore d'évaluation
- How To Import Excel Into LabviewDocument3 pagesHow To Import Excel Into LabviewDan JohnsonPas encore d'évaluation
- Xy6112 EtcDocument4 pagesXy6112 EtcJalal AsadianPas encore d'évaluation
- Carbon 06 00052Document17 pagesCarbon 06 00052Elbahi DjaalabPas encore d'évaluation