Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Handout 13 Biotechnology in Promoting Law and Order PDFDocument36 pagesHandout 13 Biotechnology in Promoting Law and Order PDFMiccah Angela Parreño FraynaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
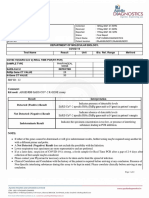
- Department of Molecular Biology. Covid 19 Test Name Result Unit Bio. Ref. Range MethodDocument2 pagesDepartment of Molecular Biology. Covid 19 Test Name Result Unit Bio. Ref. Range MethodDevi Sri PrasadPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- MQP RPQP05Document10 pagesMQP RPQP05Sheryl Cherian ParakkalPas encore d'évaluation
- Canine and Feline Infectious Diseases PDFDocument924 pagesCanine and Feline Infectious Diseases PDFGrichi86% (7)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Tobacco Mutation BreedingDocument13 pagesTobacco Mutation BreedingAnink Dwiie AnjossPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- PCR Purification QiagenDocument1 pagePCR Purification Qiagenthethoi126Pas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Occurrence of Pathogens in Raw and Ready-to-Eat Meat and Poultry Products Collected From The Retail Marketplace in Edmonton, Alberta, CanadaDocument9 pagesOccurrence of Pathogens in Raw and Ready-to-Eat Meat and Poultry Products Collected From The Retail Marketplace in Edmonton, Alberta, CanadaLolPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Quantification of Mitochondrial DNADocument5 pagesQuantification of Mitochondrial DNAKELETELA jianPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Dnase Sigma ManualDocument2 pagesDnase Sigma ManualeubacteriaPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Instruction Manual, Iscript Select cDNA Synthesis Kit, Rev BDocument2 pagesInstruction Manual, Iscript Select cDNA Synthesis Kit, Rev BdnajenPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Science and Tech Notes PDFDocument174 pagesScience and Tech Notes PDFramPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- 1876 Robert KochDocument6 pages1876 Robert KochSarah PavuPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Aspek Diagnostik MolekularDocument60 pagesAspek Diagnostik MolekularandhikaPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- MiSeq Equipment Pre-Installation ChecklistDocument5 pagesMiSeq Equipment Pre-Installation ChecklistYosep GunawanPas encore d'évaluation
- BIO203 Final Term Past PapersDocument5 pagesBIO203 Final Term Past PapersHRrehmanPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- DNA Fingerprinting 2021Document35 pagesDNA Fingerprinting 2021Makam AbhinavPas encore d'évaluation
- Lightbulb PCR Arduino CodeDocument2 pagesLightbulb PCR Arduino Codeglodovichi100% (1)
- Mesin PCR Termo Hybaid PDFDocument92 pagesMesin PCR Termo Hybaid PDFArif MulyantoPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- International Biodeterioration & Biodegradation: A B A C D ADocument10 pagesInternational Biodeterioration & Biodegradation: A B A C D ASalemPas encore d'évaluation
- Wizard Genomic DNA Purification Kit ProtocolDocument21 pagesWizard Genomic DNA Purification Kit ProtocolSri Nowo MinartiPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Intratumoral Bacterial Metataxonomic Signature of Hepatocellular CarcinomaDocument20 pagesThe Intratumoral Bacterial Metataxonomic Signature of Hepatocellular CarcinomaDenisPas encore d'évaluation
- Indoor and Outdoor Food Services Detailed GuidelinesDocument17 pagesIndoor and Outdoor Food Services Detailed GuidelinesNews 8 WROCPas encore d'évaluation
- Introduction To VirologyDocument55 pagesIntroduction To VirologymulatumelesePas encore d'évaluation
- Real-Time PCR BasicsDocument78 pagesReal-Time PCR BasicsSubbagbinfung Rumkit Bhayangkara Palangka RayaPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Antimicrobial Profile of Multidrug-Resistant Streptococcus Spp. Isolated From Dairy Cows With Clinical MastitisDocument12 pagesAntimicrobial Profile of Multidrug-Resistant Streptococcus Spp. Isolated From Dairy Cows With Clinical MastitisGezahegn BushoPas encore d'évaluation
- Lab Manual Molecular BiologyDocument19 pagesLab Manual Molecular BiologyLockerLingPas encore d'évaluation
- Foodproof Hepatitis A Virus Detection Kit: - 5 NucleaseDocument10 pagesFoodproof Hepatitis A Virus Detection Kit: - 5 NucleaseRaka AryawanPas encore d'évaluation
- COVID Is The-Virus-That-Does-Not-ExistDocument41 pagesCOVID Is The-Virus-That-Does-Not-ExistHansley Templeton Cook100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Purelink Pro 96 Rna Purification Kit: User GuideDocument28 pagesPurelink Pro 96 Rna Purification Kit: User Guidesofi garcia mendozaPas encore d'évaluation
- GMO-JRC Compendiu 2011Document259 pagesGMO-JRC Compendiu 2011Mihai IonitaPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)