1
peerEmed.com, Jan 2011
FEASIBILITY OF FIDUCIAL-FREE PRONE-POSITION TREATMENTS WITH
CYBERKNIFE FOR LOWER LUMBAR/SACRAL SPINE LESIONS
Frweger C
1,*
, Drexler C
1
, KuIeld M
1
, Wowra B
1
1
European CyberkniIe Center Munich, Germany
ABSTRACT
Objective: For spinal Cyberknife (CK) treatments, prone patient position can yield a dosimetric advantage for
posterior lesions, but the target can be subject to respiratory motion. We treated 17 lower lumbar/sacral lesions in
prone position using CK fiducial-free Xsight
TM
spine tracking and analyzed motion data in order to establish an
adequate margin concept. Methods: The lumbar spine and pelvis were elevated and stabilized to decouple the
target from respiration. The tracking region of interest was centered at the lumbar vertebrae L4/L5. Pairs of X-ray
images were taken periodically (1.4 per minute) during treatment. Tracking data from two periods of 6 to 15
minutes per treatment were analyzed to assess the extent of breathing-induced motion. Results: Stochastic motion
in left/right and superior/inferior direction was small, with peak amplitudes of 0.400.20 mm and 0.580.31 mm.
Anterior/posterior spine motion was significantly increased with a peak amplitude of 1.270.50 mm, and was
positively correlated with a head-down/-up tilt of the spine due to breathing. Conclusions: Fiducial-free prone
treatments of the lower lumbar and sacral spine are feasible using Xsight
TM
spine tracking and proper
immobilization. The residual impact of respiratory motion can be compensated with an additional PTV margin of 3
mm.
INTRODUCTION
Spinal stereotactic radiosurgery is an increasingly adopted
technique (1) that relies on highly accurate delivery oI large
radiation doses to spinal lesions. For this purpose, diIIerent
image-guidance methods are applied in order to minimize
the geometric targeting error. While, initially, Iiducial
implants were required Ior image-guidance (2), current
technology alternatively uses the skeletal structure oI the
spine as positional reIerence (3, 4, 5).
The current CyberKniIe version (CK, Accuray Inc.,
Sunnyvale, CA) has recently been described in a
comprehensive review (6). BrieIly, it is comprised oI a
compact linear accelerator mounted on a robotic arm, and a
stereoscopic kV imaging system. For image-guided
delivery oI CK treatments, diIIerent soItware applications
are used to identiIy the target and to correct the robot
position with respect to the current target location.
The CK system is capable oI precisely delivering
treatments consisting oI a large number (~100) oI non-
isocentric, non-coplanar beams Irom a large solid angle
around the patient. However, due to the speciIics oI the CK
conIiguration, the space below the treatment table cannot
be accessed by the linac, which prohibits posterior radiation
beams Ior patients in supine position. As a consequence,
treatment oI spinal targets in prone position suggests a
potential advantage in terms oI total dose and dose to
speciIic organs at risk (e.g. bowel) as well as a reduction in
monitor units, provided that additional spine motion due to
respiration is adequately managed.
Given the available image-guidance modalities, there are
two diIIerent ways to treat spinal lesions with CK: First,
Iiducial tracking, which uses radio-opaque markers (such as
screws) attached to the spine and is supported by the
manuIacturer Ior both prone (additionally using the
Synchrony system Ior compensation oI respiratory motion)
and supine position (7). Second, Iiducial-Iree Xsight spine
tracking (XST), which uses the skeletal structure oI the
spine as reIerence, but is not designed to work in
combination with the Synchrony system. XST is thereIore
supported by the manuIacturer Ior supine treatments only
(7).
For lesions in the lower lumbar and sacral spine, the CK
user is leIt with two recommended options: Invasive
implantation oI Iiducials Ior prone position treatment, or
XST in supine position, at the cost oI additional dose to the
pelvis. However, despite oI prone position, respiration-
induced movement oI the lower lumbar and sacral spine is
low in comparison to the upper lumbar or thoracic spine. It
can Iurther be reduced by using proper immobilization
techniques. We have thereIore perIormed 17 prone-position
treatments using CK Xsight spine tracking Ior targeting the
lower lumbar and sacral spine in order to demonstrate the
Ieasibility oI this technique. We have analyzed spine
motion patterns during treatment to establish and veriIy an
appropriate margin concept.
Figure 1. Prone setup example. A vacuum cushion was
used to elevate the pelvis. For treatment, a belt was used
for additional stabili:ation (upper right, grev belt not vet
fastened).
METHODS
Xsight Spine Tracking (XST)
The Xsight spine tracking system (8) matches stereoscopic
live images oI the spinal region oI interest (ROI) with
synthetic reIerence images (digitally reconstructed
radiographs DRRs) to determine the position oI the spinal
*Corresponding author: christoph.Iuerwegercyber-kniIe.net
FRWEGER ET AL.
2
target. The ROI typically includes three to Iour adjacent
vertebrae. Stereoscopic live images are acquired
periodically during treatment to continuously update the
positional inIormation. This data is utilized to redirect the
incident beams to the current location oI the spinal target by
automatically adapting the position oI the robotic arm. For
supine treatments, the XST system has been demonstrated
to achieve a clinical accuracy oI less than 1 mm despite oI
intraIraction patient motion (9).
Prone Patient Treatments
A prone position helical CT scan was acquired with 1 mm
slice thickness Ior dose planning and calculation oI DRRs.
Since the CK soItware prohibits XST tracking Ior prone
planning CT scans, they were designated as "supine"
despite oI patient prone position, As a consequence,
leIt/right and anterior/posterior directions oI the dataset are
reversed. For scanning, the pelvis was elevated and
stabilized using a vacuum cushion, pads and a belt Ior
Iixation (Iig. 1), as needed. In this manner, we aimed to
decouple the anatomy to be treated Irom respiratory
motion. An individually optimized position with minimal
motion was identiIied Ior each patient. The extent oI
residual motion in the lower lumbar/sacral spine was
visually checked by a physician and a physicist
immediately beIore CT scanning. The Iinal patient position
was careIully documented in order to correctly reproduce
the setup Ior treatment.
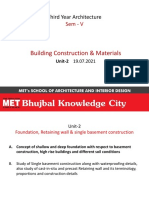
Figure 2. Data analvsis for a single observation period of 15 minutes. Translational directions inferior/superior (I/S),
left/right (L/R) and anterior/posterior (A/P) are given. A (left). Translational raw data as a function of time. This patient
shows a pronounced drift in L/R and comparablv minor drifts in I/S and A/P directions, as indicated bv least square linear
fits. Overall, the extent of svstematic drift is above average for this example case. B (right). Stochastic motion as a
function of time. Bv subtracting the drift, the stochastic component is isolated. For this patient, excursions in A/P direction
are predominant.
FRWEGER ET AL.
3
Patients were treated in prone position Ior a median
treatment time oI 95 minutes. This timeIrame typically
included one or two treatment breaks oI a Iew minutes. The
tracking ROI was centered at lumbar spine 4/5. For sacral
lesions, tracking on the lower lumbar spine has been
demonstrated to yield adequate accuracy (10). X-ray
images were acquired during treatment every 1 to 3 non-
blocked beams. The ROI in each image pair was matched
with the corresponding DRRs and the positional deviations
were recorded as a 6-dimensional vector with 3
translational (superior/inIerior, leIt/right, anterior/posterior)
and 3 rotational components (roll, pitch, yaw).
Data Analysis
We analyzed motion data in all 6 degrees oI Ireedom Ior 17
single-Iraction treatments. For each treatment, two periods
oI 6 to 15 minutes (mean 13.9) without manual couch
repositioning were isolated Ior analysis oI motion patterns
(Iig.2A). On average, 19 image pairs were acquired during
each observation period, which corresponds to a mean
image Irequency oI 1.4 images per minute.
Patient motion patterns are composed oI a non-random
driIt component overlaid by stochastic shiIts (11, 12). Since
each X-ray acquisition represents a 'snap-shot oI a
random phase in the breathing cycle, the respiration-
induced target motion is included in the stochastic
component. We thereIore separated and subtracted the
target driIt in order to assess the extent oI breathing-
induced motion, using the Iollowing simpliIied Iormalism:
For each observation period, the driIt component can be
described by a least square linear Iit oI the positional data
as a Iirst-order approximation (Iig. 2A). This driIt was
quantiIied and subtracted Irom the raw data to isolate the
stochastic part (Iig. 2B). The peak amplitude A oI the
stochastic component (n data points) Ior translation x was
calculated according to
A =
mux(x
1
..x
n
)-mn(x
1
..x
n
)
2
(1)
By this deIinition, A includes both respiration-induced
positional shiIts as well as truly stochastic motion. When
the respiratory component is predominant this value
represents a measure Ior the extent oI breathing-induced
residual motion in a speciIic direction.
RESULTS
All patients tolerated treatments in prone position
reasonably well. By allowing Ior treatment breaks upon
request, all patients were able to maintain this position
despite oI prolonged treatment times. Xsight spine tracking
could be perIormed with no indication oI a regional
mismatch.
The mean stochastic motion in leIt/right and
superior/inIerior direction was small, with peak amplitudes
oI 0.40+0.20 mm (median: 0.46 mm) and 0.58+0.31 mm
(median: 0.50 mm), respectively (Iig. 3). The major
contribution to overall stochastic motion was Irom the
anterior/posterior direction, where signiIicantly increased
shiIts with a mean peak amplitude oI 1.27+0.50 mm
(median: 1.21 mm) were observed (Iig. 3). The extent oI
anterior/posterior motion was subject to a large patient-
speciIic variation, with a minimum value oI 0.38 mm and a
maximum oI 2.29 mm.
Anterior/posterior stochastic motion was positively
correlated with a head-down/-up tilt oI the spine in 15 out
oI 17 cases, with a mean rotation oI 0.24+0.07 Ior 1 mm oI
translational excursion. Fig. 4 shows two observation
periods Ior a single sample case with a pronounced
connection oI pitch and anterior/posterior motion. Roll and
yaw rotations changed independently Ior all cases, with no
correlation with translational shiIts.
Figure 3. Box-whisker-plots of peak amplitude A for
stochastic motion in the three translational degrees of
freedom.
The median driIt over 10 minutes was 0.29 mm along the
inIerior/superior, 0.57 mm along the leIt/right and 0.64 mm
along the anterior/posterior axis (Iig. 5). The median total
translational driIt (RMS) was 1.08 mm. Only Ior two
patients, a total driIt oI more than 3 mm was encountered
over the 10 minute timeIrame (Iig. 5).
Figure 4. Anterior/posterior (A/P) motion vs. pitch. Two
observations periods (11.2 and 14.8 minutes) of a sample
case are given. A linear correlation (Pearsons coefficient
r 0.71 for the turquoise and 0.74 for the brown plot) was
observed. On average, 1 mm anterior/posterior motion
corresponded to a spine tilt of 0.29 for this patient.
FRWEGER ET AL.
4
DISCUSSION
We adopted a prone setup technique intended to stabilize
the target spine region. The applied immobilization
measures were Iound to allow Ior small driIts in position
during treatment. Hoogeman et al. (11) reported a mean
driIt (RMS) oI 1.2 mm over 15 minutes Ior extracranial
supine treatments and 2.2 mm Ior prone position,
respectively. In comparison, our data lies almost exactly in
the middle oI these two values, which is evidence that our
patient setup is adequately stable.
Figure 5. Box- whisker-plots of the translational drift per
10 minutes. Outliers are indicated.
In terms oI the stochastic component, prone patient
position resulted in substantial amount oI motion in
anterior/posterior direction, which signiIicantly exceeded
movement along the leIt/right (p7.4x10
-5
, paired student t-
test) and superior/inIerior (p9.1x10
-7
, paired student t-test)
axes. The pronounced correlation with spine pitch is
indication that the anterior/posterior motion oI the lumbar
/sacral spine was not oI a strictly 'stochastic nature, but
was mainly induced by movement oI the abdomen and/or
chest due to breathing.
Even though the tracking region oI interest was always
centered on the same vertebrae, the extent and
characteristics oI observed motion patterns during treatment
were very diverse. Furthermore, we experienced one case
oI a patient who could not be adequately stabilized already
during CT scanning, despite our best eIIorts. ThereIore, this
patient was not selected Ior treatment in in prone position.
In our experience, the individual patient anatomy is the key
Iactor that determines whether prone treatment is advisable,
and which immobilization measures are most successIul. In
particular, obese patients with a large abdominal girth are
diIIicult to stabilize. Close monitoring and reIining oI setup
procedures by expert personnel is crucial Ior patient saIety.
Finally, we want to deduce a suitable PTV margin to
account Ior the additional uncertainty. In a DVH-based
approach, van Herk et al. (13) have derived a simple
Iormula Ior calculation oI margins. They distinguish
between 'preparation errors causing a systematic shiIt and
stochastic 'execution errors causing a blurring oI the dose
distribution. For a multiple Iraction treatment, a standard
CTV-to-PTV margin m
PTJ
can then be approximated by
m
P1v
= 2.S2 + u.7o (2)
which corresponds to 95 coverage Ior 90 oI the
patients and a width oI 3.2 mm Ior the penumbra.12 and 3
reIer to the standard deviations oI preparation and
execution errors (13).
This recipe has been derived assuming multiple Iractions,
where the average oI the random error over the whole
treatment course is zero. This assumption is not IulIilled Ior
single-Iraction CK treatments, and thereIore, eq. |2| is not
directly applicable. However, Hoogeman et al. (11) have
adopted the Iormalism to estimate a margin applicable to
single Iraction, image-guided treatments by using the
standard deviation oI the intraIraction driIt as the
systematic error 2 and the standard deviation oI the
stochastic motion component as 3. We Iollowed their
approach and used our driIt and stochastic motion data as
input parameters. Based on the average Irequency oI 1.4
stereoscopic image acquisitions per minute Ior our
observation periods, we assumed a longer imaging interval
oI 1 minute as a conservative estimate. With these values,
we calculated a value oI 0.10 mm Ior 24 A value oI 1.58
mm was determined Ior 3, assuming sinusoidal stochastic
motion with the measured peak amplitudes A. Using eq. |2|,
m
PTJ
amounts to 1.4 mm.
Up to this point, the impact oI rotations as a potential
source oI error has been neglected in the calculation oI m
PTJ
(13). Respiration-induced pitch motion and residual
stochastic rotations add to the uncertainty. A distance oI up
to 6 cm between the center oI the tracking ROI and the
lesion, which is representative Ior lumbar/sacral targets,
and a conservative estimate oI 1 degree Ior the rotational
error correspond to an additional targeting error oI up to 1
mm on top oI the value calculated with translations only.
We thereIore recommend and have chosen to apply a
uniIorm margin oI 3 mm to assure adequate target
coverage.
In comparison, CK spinal treatments in supine position
can be perIormed with submillimeter accuracy (9), with no
need Ior an additional margin. Since, eIIectively, a larger
target must be treated in prone position, this countervails a
potential dosimetric advantage due to shorter beam paths.
Furthermore, a new optimized supine setup technique using
a thick Ioam pad improves lateral access with the CK (14),
which can also be beneIicial Ior posterior lesions in the
lumbar/sacral spine. In order to develop clear patient
selection criteria Ior prone treatment in the Iuture, a
comparative planning study is needed. This study must
include diIIerent margins to correctly account Ior target
motion.
CONCLUSIONS
We have demonstrated the Ieasibility oI Iiducial-Iree prone
treatments in the lower lumbar and sacral spine, thus Iurther
extending the usability oI the CyberKniIe. When suitable
immobilization techniques are applied, the target motion
due to breathing can be limited to a Iew millimeters overall.
This can be compensated by a slightly increased size oI the
PTV, which must be careIully weighed against a presumed
dosimetric beneIit due to posterior radiation access.
REFERENCES
1.1 Hsu W, Nguyen T, Kleinberg L, Ford EC, Rigamonti D,
Gokaslan ZL, Lim M. Stereotactic radiosurgery Ior
spine tumors: review oI current literature. Stereotact
Funct Neurosurg. 2010;88(5):315-21. Epub 2010 Aug
13.
2.1 Gerszten PC, Burton SA. Clinical assessment oI
stereotactic IGRT: spinal radiosurgery. Med Dosim
2008;33:107-116.
3.1 Agazaryan N, Tenn SE, Desalles AA, Selch MT.
Image-guided radiosurgery Ior spinal tumors: methods,
accuracy and patient intraIraction motion. Phys Med
Biol 2008;53:1715-1727.
FRWEGER ET AL.
5
4.1 Chang Z, Wang Z, Ma J, O'Daniel JC, Kirkpatrick J,
Yin FF. 6D image guidance Ior spinal non-invasive
stereotactic body radiation therapy: Comparison
between ExacTrac X-ray 6D with kilo-voltage cone-
beam CT. Radiother Oncol. 2010 Apr;95(1):116-21.
Epub 2010 Feb 1.
5.1 Muacevic A, Staehler M, Drexler C, Wowra B, Reiser
M, Tonn JC. Technical description, phantom accuracy,
and clinical Ieasibility Ior Iiducial-Iree Irameless real-
time image-guided spinal radiosurgery. J Neurosurg
Spine 2006;5:303-312.
6.1 Kilby W, Dooley JR, Kuduvalli G, Sayeh S, Maurer CR
Jr. The CyberKniIe Robotic Radiosurgery System in
2010. Technol Cancer Res Treat. 2010 Oct;9(5):433-52.
7.1 Accuray Inc., Sunnyvale, CA, USA. Treatment Delivery
Manual, CyberKniIe version 8.5.x. 2009.
8.1 Ho AK, Fu D, Cotrutz C, Hancock SL, Chang SD,
Gibbs IC, Maurer CR, Adler JR. A study oI the
accuracy oI CyberkniIe spinal radiosurgery using
skeletal structure tracking. Neurosurgery 2007;60:147-
156.
9.1 Frweger C, Drexler C, KuIeld M, Muacevic A, Wowra
B, SchlaeIer A. Patient Motion and Targeting Accuracy
in Robotic Spinal Radiosurgery: 260 Single-Fraction
Fiducial-Free Cases. Int J Radiat Oncol Biol Phys. 2010
Nov 1;78(3):937-45. Epub 2010 Apr 13.
10.1Muacevic A, Drexler C, KuIeld M, Romanelli P, Duerr
HJ, Wowra B. Fiducial-Iree real-time image-guided
robotic radiosurgery Ior tumors oI the sacrum/pelvis.
Radiother Oncol. 2009 Oct;93(1):37-44. Epub 2009 Jun
22.
11.1Hoogeman MS, Nuyttens JJ, Levendag PC, Heijmen
BJM. Time dependence oI intraIraction patient motion
assessed by repeat stereoscopic imaging. Int J Radiat
Oncol Biol Phys 2008;70:609-618.
12.1Ma L, Sahgal A, Hossain S, Chuang C, Descovich M,
Huang K, Gottschalk A, Larson DA. Nonrandom
intraIraction target motions and general strategy Ior
correction oI spine stereotactic body radiotherapy. Int J
Radiat Oncol Biol Phys. 2009 Nov 15;75(4):1261-5.
Epub 2009 Aug 3.
13.1Van Herk M, Remeijer P, Lebesque JV. Inclusion oI
geometric uncertainties in treatment plan evaluation. Int
J Radiat Oncol Biol Phys. 2002 Apr 1;52(5):1407-22.
14.1Hevezi JM. A new patient support pad Ior CyberKniIe
planning & delivery - a technical note.
http.//www.peeremed.com. Epub 2010 Oct 28.
Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Epidemiology of Angioid Streaks-Associated Choroidal Neovascular Membranes in The United KingdomDocument20 pagesEpidemiology of Angioid Streaks-Associated Choroidal Neovascular Membranes in The United KingdomCureusPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Musculosleketal Risk Assesment Among Nurses in Pateint Manual Handling in Hospital Wards - A Cross Sectional StudyDocument10 pagesMusculosleketal Risk Assesment Among Nurses in Pateint Manual Handling in Hospital Wards - A Cross Sectional StudyCureusPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Oncothermia: A New Paradigm in Cancer TherapiesDocument31 pagesOncothermia: A New Paradigm in Cancer TherapiesCureus100% (1)
- Outcome of Wearing High Heel Shoes in Young GenerationDocument16 pagesOutcome of Wearing High Heel Shoes in Young GenerationCureusPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Cardiac Radiosurgery (CyberHeart™) For Treatment of Arrhythmia: Physiologic and Histopathologic Correlation in The Porcine ModelDocument28 pagesCardiac Radiosurgery (CyberHeart™) For Treatment of Arrhythmia: Physiologic and Histopathologic Correlation in The Porcine ModelCureusPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Dizziness, Postural Blackouts? - It Could Be Multiple System Atrophy.Document5 pagesDizziness, Postural Blackouts? - It Could Be Multiple System Atrophy.CureusPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Nursing Care Plan HydrocephalusDocument7 pagesNursing Care Plan HydrocephalusFarnii MarquezPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Year 8 Mid-Term Maths TestDocument7 pagesYear 8 Mid-Term Maths TestJenniferPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Western Desert Versus Nile Delta A C PDFDocument17 pagesThe Western Desert Versus Nile Delta A C PDFSohini ChatterjeePas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Haynes 230 Alloy: Principal FeaturesDocument28 pagesHaynes 230 Alloy: Principal FeaturesMatheus DominguesPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- 12Document11 pages12ANK SHRINIVAASAN100% (1)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Agricultural Crop ProductionDocument10 pagesAgricultural Crop ProductionElisha Liwag100% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Practical Acoustics of Instruments of The Violin FamilyDocument13 pagesPractical Acoustics of Instruments of The Violin Familyapi-287441447100% (1)
- Point Schedule BAS - LAVENUE - r2Document10 pagesPoint Schedule BAS - LAVENUE - r2Quantum SalesPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Climate Change in The Philippines PDFDocument44 pagesClimate Change in The Philippines PDFlipPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Vocabulary of Analytical Chemistry: Chapter OverviewDocument22 pagesThe Vocabulary of Analytical Chemistry: Chapter OverviewAwash TinsaePas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Maximalist NovelDocument16 pagesThe Maximalist Novelosirx277100% (2)
- BCM-V U2 Part-A 19-07-2021Document21 pagesBCM-V U2 Part-A 19-07-2021hyperloop707 designPas encore d'évaluation
- C7000/6000 Icp List: Konica Minolta Confidential HQ Uses OnlyDocument18 pagesC7000/6000 Icp List: Konica Minolta Confidential HQ Uses OnlyJorge Cazana100% (1)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Environmental AssessmentDocument119 pagesEnvironmental AssessmentSarahLukakuPas encore d'évaluation
- J. Electrochem. Soc. 1954 Belle 339 42Document4 pagesJ. Electrochem. Soc. 1954 Belle 339 42Sutanwi LahiriPas encore d'évaluation
- The Aeroponic SystemDocument15 pagesThe Aeroponic SystemLiviu AngelescuPas encore d'évaluation
- Project Proposal Form (Edexcel) 2Document3 pagesProject Proposal Form (Edexcel) 2Максим КарплюкPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- Arul MuruganDocument2 pagesArul Muruganaravindpersonal07Pas encore d'évaluation
- Eyes of Nye - Human PopulationDocument3 pagesEyes of Nye - Human Populationmakenziee j .Pas encore d'évaluation
- Chinese Characters Confirm Christian Concept (Revised)Document6 pagesChinese Characters Confirm Christian Concept (Revised)Sammy Lee100% (1)
- Food (Fish) Processing: Washing and Sterilizing of Packaging MaterialsDocument20 pagesFood (Fish) Processing: Washing and Sterilizing of Packaging MaterialsMaria Rose Tariga AquinoPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- DGDocument7 652 pagesDGNaga NitheshPas encore d'évaluation
- PSRIG LiftingDocument12 pagesPSRIG LiftingCristinaHernándezPas encore d'évaluation
- Beginning CosmodynesDocument2 pagesBeginning CosmodynesDilip KiningePas encore d'évaluation
- KVR Price List: SL - No Particulars UnitsDocument32 pagesKVR Price List: SL - No Particulars UnitsSudharshanPas encore d'évaluation
- Chapter IV Kaivalya PådaDocument5 pagesChapter IV Kaivalya PådaAnonymous gqSpNAmlWPas encore d'évaluation
- (Pro-Forma) : WHEREAS, The RE Developer Is Authorized To Proceed To The Development Stage of Its RenewableDocument13 pages(Pro-Forma) : WHEREAS, The RE Developer Is Authorized To Proceed To The Development Stage of Its RenewableJoy AlamedaPas encore d'évaluation
- Philippine Navy Enlisted Rating Structure: Military Science (Ms-2)Document10 pagesPhilippine Navy Enlisted Rating Structure: Military Science (Ms-2)Kristine AquitPas encore d'évaluation
- Englisch LK MediationDocument1 pageEnglisch LK Mediation5m2yjn778sPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)