Vous aimerez peut-être aussi
- LG RN Ad For WebDocument1 pageLG RN Ad For WebbagsikPas encore d'évaluation
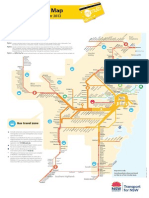
- Mymulti Fare MapDocument1 pageMymulti Fare Maphoneytrap99Pas encore d'évaluation
- Visit Transportnsw - Info: Description of Routes in This Timetable Route 611Document11 pagesVisit Transportnsw - Info: Description of Routes in This Timetable Route 611bagsikPas encore d'évaluation
- Am J Crit Care 2008 Chang 408 15Document10 pagesAm J Crit Care 2008 Chang 408 15bagsikPas encore d'évaluation
- NANDA NursingDocument159 pagesNANDA NursingAijem RyanPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Acute Asthma Paed WaniDocument16 pagesAcute Asthma Paed WaniNurul Syazwani RamliPas encore d'évaluation
- Soal Bahasa Inggris 2aDocument19 pagesSoal Bahasa Inggris 2aMegaaPas encore d'évaluation
- Bulk Forming PurgativesDocument12 pagesBulk Forming PurgativesabcdPas encore d'évaluation
- Distinct Spectrum of CFTR Gene MutationsDocument13 pagesDistinct Spectrum of CFTR Gene Mutationsapi-3742014Pas encore d'évaluation
- Prolapsed Intervertebral Disc: By: Diksha Solanki Bot 4 YearDocument37 pagesProlapsed Intervertebral Disc: By: Diksha Solanki Bot 4 YearISIC IRS100% (1)
- Envidea 2011 ASP Case StudyDocument17 pagesEnvidea 2011 ASP Case Studylefty298Pas encore d'évaluation
- Hemolytic Disease of The Fetus and NewbornDocument6 pagesHemolytic Disease of The Fetus and NewbornCj CCPas encore d'évaluation
- 1 s2.0 S2772594422001637 MainDocument5 pages1 s2.0 S2772594422001637 MainCatarina CourasPas encore d'évaluation
- SAMPLE Outline PanicDocument3 pagesSAMPLE Outline PanicdexPas encore d'évaluation
- Spinal StenosisDocument14 pagesSpinal StenosisHONGJYPas encore d'évaluation
- Knowledge On Risk Factors of Diabetes Mellitus 2 Among Students in Selected Universities in RwandaDocument6 pagesKnowledge On Risk Factors of Diabetes Mellitus 2 Among Students in Selected Universities in RwandaInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- 79 Endotracheal IntubationDocument1 page79 Endotracheal IntubationAdria Putra FarhandikaPas encore d'évaluation
- Limfadenitis Akut Dan KronisDocument24 pagesLimfadenitis Akut Dan KronisRezy Pysesia AlfaniPas encore d'évaluation
- NCM 3114 Acid Base Imbalance-2Document13 pagesNCM 3114 Acid Base Imbalance-2Fayeh Harah PadrillanPas encore d'évaluation
- Aedes Egypti ADocument10 pagesAedes Egypti AOswin YohsaPas encore d'évaluation
- Acta Pediatrica Enero 2021 - Topicos NeonatalesDocument113 pagesActa Pediatrica Enero 2021 - Topicos NeonatalesalbertoPas encore d'évaluation
- Contents of Wetland Medicinal Plants in Taiwan: Antioxidant Properties and Total PhenolicDocument12 pagesContents of Wetland Medicinal Plants in Taiwan: Antioxidant Properties and Total Phenolicvaishali shuklaPas encore d'évaluation
- Janberidze Et Al 2015Document10 pagesJanberidze Et Al 2015Elene JanberidzePas encore d'évaluation
- Drug - WikipediaDocument4 pagesDrug - WikipedianightmarePas encore d'évaluation
- Clinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test BankDocument9 pagesClinical Manifestations and Assessment of Respiratory Disease 5th Edition Jardins Test Banksarahpalmerotpdkjcwfq100% (26)
- Biology Notes (Bilingual)Document349 pagesBiology Notes (Bilingual)dipanjan biswasPas encore d'évaluation
- Effects of Longterm Ritalin UseDocument4 pagesEffects of Longterm Ritalin Usebellydanceafrica9540Pas encore d'évaluation
- OsteoarthritisDocument4 pagesOsteoarthritisDharti PatelPas encore d'évaluation
- Does WiFi Affect The BrainDocument6 pagesDoes WiFi Affect The BrainrustyPas encore d'évaluation
- Sr. No. Cghs Treatment Procedure/Investigation List Non-NABH/Non - NABL Rates Nabh/Nabl RatesDocument49 pagesSr. No. Cghs Treatment Procedure/Investigation List Non-NABH/Non - NABL Rates Nabh/Nabl RatesADDECC INFO INDIAPas encore d'évaluation
- Jessica Delcourt 102503542 WallDocument2 pagesJessica Delcourt 102503542 Wallapi-558053325Pas encore d'évaluation
- Discussion Question 1Document3 pagesDiscussion Question 1Brian RelsonPas encore d'évaluation
- Pediatric BLSDocument32 pagesPediatric BLSYuni AjahPas encore d'évaluation
- Video Recap of Mutations by Amoeba SistersDocument2 pagesVideo Recap of Mutations by Amoeba Sistersapi-233187566Pas encore d'évaluation
- Speaking Part 3 Update 2022Document7 pagesSpeaking Part 3 Update 2022Nhi LêPas encore d'évaluation