Vous aimerez peut-être aussi
- RECTAL BLEEDING HISTORYDocument7 pagesRECTAL BLEEDING HISTORYShalini Shanmugalingam100% (1)
- Common General Practice Consultations - Notes For OSCEsDocument54 pagesCommon General Practice Consultations - Notes For OSCEshaydenfarquhar89% (9)
- Mnemonics For Clinical ExamDocument20 pagesMnemonics For Clinical ExamDrAmeen1976100% (3)
- The Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesD'EverandThe Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesPas encore d'évaluation
- KHALIL High Yeild Step 2 CS Mnemonic-COLORDocument10 pagesKHALIL High Yeild Step 2 CS Mnemonic-COLORPratap Tetali100% (2)
- Osce Bank PDFDocument15 pagesOsce Bank PDFnassir197083% (6)
- MRCGP Int OsceDocument81 pagesMRCGP Int OsceAbdelnasir Abbas Abdalla ELsheikh100% (3)
- Osce Pro III Trial AnswerDocument69 pagesOsce Pro III Trial AnswerDr Onn Azli Puade100% (3)
- OSCE SkillsDocument9 pagesOSCE SkillsgoodbyetherePas encore d'évaluation
- Alphabetical List of Past PLAB Part 2 OSCE Stations PLAB Part 2Document7 pagesAlphabetical List of Past PLAB Part 2 OSCE Stations PLAB Part 2jahangirealam100% (1)
- OSCE EverythingDocument24 pagesOSCE EverythingkendymillPas encore d'évaluation
- Clinical OSCE NotesDocument49 pagesClinical OSCE Notesrandom.mail.scsm711250% (2)
- Osce Revision Questions 2017Document21 pagesOsce Revision Questions 2017Leong Tung OngPas encore d'évaluation
- Family Medicine - General Practice MEQ 2006Document6 pagesFamily Medicine - General Practice MEQ 2006jermie22100% (1)
- OSCE Guide, University of Queensland School of MedicineDocument86 pagesOSCE Guide, University of Queensland School of MedicineDarren Pang100% (2)
- PLAB 2 Notes Part 2Document565 pagesPLAB 2 Notes Part 2Anonymous YqCxXQ6wF5Pas encore d'évaluation
- The Resident's Guide To LMCC II (And MCC Qualifying Exam II)Document56 pagesThe Resident's Guide To LMCC II (And MCC Qualifying Exam II)bobsherif86% (7)
- A Step by Step Guide To Mastering The OSCEsDocument20 pagesA Step by Step Guide To Mastering The OSCEsAl Imari60% (10)
- Symptoms Differential ChartsDocument52 pagesSymptoms Differential ChartsXiaxin Liu100% (2)
- Osce Book 3rdDocument39 pagesOsce Book 3rdأحمد الكندي100% (1)
- Dr Arora's Communication Skills for Patient ConsultationsDocument5 pagesDr Arora's Communication Skills for Patient Consultationsy æsk100% (2)
- Osce MedDocument58 pagesOsce MedYS Nate100% (1)
- Fracp Osce HandbookDocument163 pagesFracp Osce HandbookTaha MohamedPas encore d'évaluation
- Clinical OSCE Notes PDFDocument49 pagesClinical OSCE Notes PDFArwa QishtaPas encore d'évaluation
- Differential DiagnosisDocument41 pagesDifferential Diagnosispranjl100% (2)
- Nilo S ManikinsDocument50 pagesNilo S ManikinsKhan Zahid100% (2)
- Ace The OSCE2 BookDocument126 pagesAce The OSCE2 BookVijay Mg100% (5)
- PLAB Part 2 Is Not A Difficult Exam!!! PLAB Part 2Document9 pagesPLAB Part 2 Is Not A Difficult Exam!!! PLAB Part 2jahangirealam100% (1)
- Fitz Abdominal Paces NotesDocument19 pagesFitz Abdominal Paces NotesDrShamshad Khan100% (1)
- Urological History Taking FrameworkDocument5 pagesUrological History Taking FrameworkahmadPas encore d'évaluation
- How To Interpret CXRs For OSCEsDocument2 pagesHow To Interpret CXRs For OSCEsPrarthana Thiagarajan100% (9)
- Plab 2 PDFDocument18 pagesPlab 2 PDFSualeha SohailPas encore d'évaluation
- Sim ManDocument2 pagesSim ManTabinda Sarwar50% (2)
- Long case format and data for MBBS final examDocument110 pagesLong case format and data for MBBS final examwhee182Pas encore d'évaluation
- MRCGP Int OsceDocument39 pagesMRCGP Int OsceAbdelnasir Abbas Abdalla ELsheikh100% (6)
- Family Medicine Guide for Common ConditionsDocument42 pagesFamily Medicine Guide for Common ConditionsRojelle LezamaPas encore d'évaluation
- These Are The Stations For 14th June 2016 Plab 2 ExamDocument8 pagesThese Are The Stations For 14th June 2016 Plab 2 Examwagica100% (1)
- List of OSCE Stations in Past Six Months in PLAB Part 2 PLAB Part 2Document12 pagesList of OSCE Stations in Past Six Months in PLAB Part 2 PLAB Part 2jahangirealam100% (1)
- OSCE Clinical Examination GuideDocument109 pagesOSCE Clinical Examination Guidekhairul amilin83% (6)
- Marwa Badr Notes CSADocument44 pagesMarwa Badr Notes CSAMarwa Badr100% (1)
- Plab 2 Stations Beta VersionDocument52 pagesPlab 2 Stations Beta VersionVijay Mg75% (4)
- A Brief Sample Content of The " PACING THE PACES Tips For Passing MRCP and Final MBBS"Document24 pagesA Brief Sample Content of The " PACING THE PACES Tips For Passing MRCP and Final MBBS"Woan Torng100% (2)
- Family Medicine NotesDocument52 pagesFamily Medicine NotesGene Paolo Janzi SaplaPas encore d'évaluation
- Psychiatry Notes and Other Stations Including PCP and Dry CoughDocument66 pagesPsychiatry Notes and Other Stations Including PCP and Dry CoughMuhammad Ali50% (2)
- Osce Summary - SystemsDocument9 pagesOsce Summary - Systemsnmc_nguyen82100% (6)
- Samson Handbook of PLAB 2 and Clinical AssessmentD'EverandSamson Handbook of PLAB 2 and Clinical AssessmentÉvaluation : 4.5 sur 5 étoiles4.5/5 (8)
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionD'EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionPas encore d'évaluation
- International Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessD'EverandInternational Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessRaghav GovindarajanPas encore d'évaluation
- CLINICAL HISTORY AND DIFFERENTIAL DIAGNOSIS AT YOUR FINGERTIPSD'EverandCLINICAL HISTORY AND DIFFERENTIAL DIAGNOSIS AT YOUR FINGERTIPSPas encore d'évaluation
- A Brief Introduction to the Multi-Specialty Recruitment Assessment (MSRA)D'EverandA Brief Introduction to the Multi-Specialty Recruitment Assessment (MSRA)Évaluation : 5 sur 5 étoiles5/5 (1)
- Step 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionD'EverandStep 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionPas encore d'évaluation
- The 10-Minute Physical Exam: recognizing medical syndromesD'EverandThe 10-Minute Physical Exam: recognizing medical syndromesPas encore d'évaluation
- The Unofficial Guide to Passing OSCEs: Candidate Briefings, Patient Briefings and Mark SchemesD'EverandThe Unofficial Guide to Passing OSCEs: Candidate Briefings, Patient Briefings and Mark SchemesPas encore d'évaluation
- Clinical Skills Review: Scenarios Based on Standardized PatientsD'EverandClinical Skills Review: Scenarios Based on Standardized PatientsÉvaluation : 4 sur 5 étoiles4/5 (10)
- Buser2000 PDFDocument10 pagesBuser2000 PDFArun PrasadPas encore d'évaluation
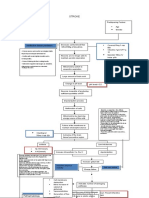
- TriageDocument37 pagesTriagekyuleen05Pas encore d'évaluation
- 2017 Boot Camp HandbookDocument98 pages2017 Boot Camp HandbookmyscribePas encore d'évaluation
- De La Salle University Medical Center Department of Obstetrics and GynecologyDocument3 pagesDe La Salle University Medical Center Department of Obstetrics and GynecologyNehemiah FranciscoPas encore d'évaluation
- Graves' Hyperthyroidism: Treatment With Antithyroid Drugs, Surgery, or Radioiodine-A Prospective, Randomized StudyDocument8 pagesGraves' Hyperthyroidism: Treatment With Antithyroid Drugs, Surgery, or Radioiodine-A Prospective, Randomized StudyRidwan Putra Beng-BengPas encore d'évaluation
- Concept Map CVADocument1 pageConcept Map CVASuzette Rae Tate100% (2)
- AmoebiasisDocument64 pagesAmoebiasisLarry MathisPas encore d'évaluation
- Unit 18 Assignment 1 (1866)Document9 pagesUnit 18 Assignment 1 (1866)Noel JenningsPas encore d'évaluation
- Lecture-18 Obstructed LaborDocument8 pagesLecture-18 Obstructed LaborMadhu Sudhan PandeyaPas encore d'évaluation
- CLAIMING FACTS, VALUES, AND POLICIESDocument3 pagesCLAIMING FACTS, VALUES, AND POLICIESPrimo100% (2)
- Autism Spectrum Disorder-MANUSCRIPT2CDocument20 pagesAutism Spectrum Disorder-MANUSCRIPT2CPaul AntePas encore d'évaluation
- Neurology Textbook for Dental StudentsDocument1 pageNeurology Textbook for Dental StudentsBelmin SalihovicPas encore d'évaluation
- Discharge Planning ProjectDocument6 pagesDischarge Planning Projectapi-282958026Pas encore d'évaluation
- PS01619 PDFDocument8 pagesPS01619 PDFEvelinaPas encore d'évaluation
- Bio Medical Waste ManagementDocument5 pagesBio Medical Waste Managementanantarao75% (4)
- Bme ReportDocument15 pagesBme ReportnikitatayaPas encore d'évaluation
- Partial Auricular ProsthesisDocument4 pagesPartial Auricular ProsthesisdrsmritiPas encore d'évaluation
- Midterm ExamDocument3 pagesMidterm Examابو سارةPas encore d'évaluation
- MSC Proposal - Quantitative - 2019Document32 pagesMSC Proposal - Quantitative - 2019Lihle Mirriam MdlalosePas encore d'évaluation
- International Journal of Scientific Research: Dental ScienceDocument2 pagesInternational Journal of Scientific Research: Dental ScienceSmart Dental ClinicsPas encore d'évaluation
- Divine Intervention Episode 17 Diseases of The Pediatric Population Part 1Document14 pagesDivine Intervention Episode 17 Diseases of The Pediatric Population Part 1Swisskelly1Pas encore d'évaluation
- Summer Diseases and Its PreventionDocument6 pagesSummer Diseases and Its PreventionJithin M Krishna EzhuthachanPas encore d'évaluation
- Perio Case StudyDocument17 pagesPerio Case Studyapi-544634047Pas encore d'évaluation
- Effectiveness of nebulized N-acetylcysteine in treating children with acute bronchiolitisDocument4 pagesEffectiveness of nebulized N-acetylcysteine in treating children with acute bronchiolitisIvan VeriswanPas encore d'évaluation
- RESPONDER Nitrile Exam GlovesDocument6 pagesRESPONDER Nitrile Exam Glovessandakelum AsankaPas encore d'évaluation
- RLE-level-2-Learning-packet-2-Blue-week-2 (Sanaani, Nur-Fatima, M.)Document29 pagesRLE-level-2-Learning-packet-2-Blue-week-2 (Sanaani, Nur-Fatima, M.)Nur SanaaniPas encore d'évaluation
- PGY2 Internal Medicine 2018Document9 pagesPGY2 Internal Medicine 2018Kilva EratulPas encore d'évaluation
- EU Harmonized Standards May 2014Document30 pagesEU Harmonized Standards May 2014ajitbasrur445Pas encore d'évaluation
- Reflection: The Nursing Act of 1991 Protecting The Public Maria Claudia Esquivel Vasquez 805 349 214Document5 pagesReflection: The Nursing Act of 1991 Protecting The Public Maria Claudia Esquivel Vasquez 805 349 214api-283154156Pas encore d'évaluation
- Humacount 5D: Outstanding 5-Part Diff Hematology SystemDocument8 pagesHumacount 5D: Outstanding 5-Part Diff Hematology SystemIndia DiscoverPas encore d'évaluation