Vous aimerez peut-être aussi
- One Step Med: General Medical Information Record Keeping ManualD'EverandOne Step Med: General Medical Information Record Keeping ManualPas encore d'évaluation
- Therapeutic Activities for Children and Teens Coping with Health IssuesD'EverandTherapeutic Activities for Children and Teens Coping with Health IssuesPas encore d'évaluation
- Heroes On Horseback Participant Registration and Photo Release FormDocument11 pagesHeroes On Horseback Participant Registration and Photo Release FormbernardhhiPas encore d'évaluation
- Special BenefitDocument20 pagesSpecial BenefitHihiPas encore d'évaluation
- Corporate Membership Application FormDocument2 pagesCorporate Membership Application Formpradhan13100% (1)
- HTD Youth Camp Medical and Consent FormDocument2 pagesHTD Youth Camp Medical and Consent FormChris BowditchPas encore d'évaluation
- AppForm - GroupMedIns - Member - 2016-06 (June14)Document3 pagesAppForm - GroupMedIns - Member - 2016-06 (June14)Ruchie EtollePas encore d'évaluation
- 2034 PDFDocument2 pages2034 PDFJagyanseni BeheraPas encore d'évaluation
- AXA Hypertension QuestionnaireDocument2 pagesAXA Hypertension QuestionnaireClaudine Limasa TabudlongPas encore d'évaluation
- Medical Application Form: Insured Name: Inception DateDocument3 pagesMedical Application Form: Insured Name: Inception DateDidier G PeñuelaPas encore d'évaluation
- HIM 200 Health RecordDocument32 pagesHIM 200 Health RecordMaryamPas encore d'évaluation
- Session 3 Registration PacketDocument4 pagesSession 3 Registration PacketASYMCA YCOPas encore d'évaluation
- Registration Forms Session 4Document4 pagesRegistration Forms Session 4ASYMCA YCOPas encore d'évaluation
- Authorization For Release of Medical InformationDocument1 pageAuthorization For Release of Medical Informationcig3fPas encore d'évaluation
- Youth Ministries Medical and Liability Release Kayaking Trip August 10Document4 pagesYouth Ministries Medical and Liability Release Kayaking Trip August 10DiaanPas encore d'évaluation
- Medical Release FormDocument1 pageMedical Release Formmr_b123Pas encore d'évaluation
- SKD Death Claim English Ver. 01Document1 pageSKD Death Claim English Ver. 01velandoPas encore d'évaluation
- Medical Examintation Report: Document No MTIPL/HR/F0006 1Document1 pageMedical Examintation Report: Document No MTIPL/HR/F0006 1Kabir ShelkePas encore d'évaluation
- Session 1 Waitlist - Registration PacketDocument4 pagesSession 1 Waitlist - Registration PacketASYMCA YCOPas encore d'évaluation
- Declaration of Medical Illness/Es (Form D) : (To Be Filled-Out by The Nominee)Document1 pageDeclaration of Medical Illness/Es (Form D) : (To Be Filled-Out by The Nominee)CHRISTIAN HARVEY WONGPas encore d'évaluation
- Uqms PirDocument2 pagesUqms PirJameslPas encore d'évaluation
- Please Return The Completed Referral Form byDocument5 pagesPlease Return The Completed Referral Form byA AkbPas encore d'évaluation
- Consent For Minor Dental PDFDocument2 pagesConsent For Minor Dental PDFJanPas encore d'évaluation
- PSRC Medical and Consent Form 20230727Document3 pagesPSRC Medical and Consent Form 20230727bigdog99bcPas encore d'évaluation
- Medicare Insurance Claim Form: PolicyholderDocument2 pagesMedicare Insurance Claim Form: PolicyholdertagashiiPas encore d'évaluation
- Medical FormDocument2 pagesMedical FormHoney AliPas encore d'évaluation
- Pre Employment Medical Declaration Form - 2022Document2 pagesPre Employment Medical Declaration Form - 2022Neel GhoshPas encore d'évaluation
- Medical Certificate 2Document2 pagesMedical Certificate 2Aditeya Shukla100% (1)
- 00000Document2 pages00000Jake CopradePas encore d'évaluation
- 2017 Day CampDocument4 pages2017 Day CampMax PlanckPas encore d'évaluation
- Medical Application Form: Name Relation (E/S/C) D. O. B SEX (M/F) Marital Status Height (CM) Weight (KG) Emirates (VISA)Document3 pagesMedical Application Form: Name Relation (E/S/C) D. O. B SEX (M/F) Marital Status Height (CM) Weight (KG) Emirates (VISA)cmthebossPas encore d'évaluation
- Medical Admission Proforma: Hospital Name Patient DetailsDocument11 pagesMedical Admission Proforma: Hospital Name Patient DetailsAngelus129Pas encore d'évaluation
- New Axa FormDocument2 pagesNew Axa FormAzrul Azuar Azrul Azuar100% (1)
- Alliance Application Form - DXB & NEDocument2 pagesAlliance Application Form - DXB & NEAnkita NiravPas encore d'évaluation
- Hospital Admission Letter Template PDFDocument1 pageHospital Admission Letter Template PDFTika Yulasni100% (5)
- YL Camping Consent and Health FormDocument4 pagesYL Camping Consent and Health Formmcronin1970Pas encore d'évaluation
- ConsentDocument2 pagesConsentNobel LaureatePas encore d'évaluation
- General Physical Examination FormDocument4 pagesGeneral Physical Examination Formecint.trmPas encore d'évaluation
- Medical Application Form PDFDocument3 pagesMedical Application Form PDFHumanPas encore d'évaluation
- Health History GirlDocument2 pagesHealth History GirlHKantesPas encore d'évaluation
- Family Health Questionnaire Form (FHQ) : Allianz EFU Health Insurance Limited Window Takaful OperationsDocument2 pagesFamily Health Questionnaire Form (FHQ) : Allianz EFU Health Insurance Limited Window Takaful OperationsnomiabbasiPas encore d'évaluation
- Medical CertificateDocument2 pagesMedical CertificatelekacaPas encore d'évaluation
- Event WaiversDocument2 pagesEvent WaiverskingdeveshPas encore d'évaluation
- Envelope - Medical Application Form - New - V3 - Mednet - 1Document3 pagesEnvelope - Medical Application Form - New - V3 - Mednet - 1muhdm7771Pas encore d'évaluation
- Claims Aps Hi MR SurgicalDocument3 pagesClaims Aps Hi MR SurgicalRudolf CunananPas encore d'évaluation
- QR-RCP-009 Authorization For Disclosure of Health InformationRecords - Rev07Document1 pageQR-RCP-009 Authorization For Disclosure of Health InformationRecords - Rev07Yel BPas encore d'évaluation
- S - A Camp Application: Ummer in MericaDocument7 pagesS - A Camp Application: Ummer in MericaHưng Thịnh NguyễnPas encore d'évaluation
- Clal Health Insurance Company LTD.: Healthy & SureDocument4 pagesClal Health Insurance Company LTD.: Healthy & SureM.I. BdaPas encore d'évaluation
- New Patient Information Form 2Document2 pagesNew Patient Information Form 2Marcela CamposPas encore d'évaluation
- Briettavasser Job 33 Form 3Document1 pageBriettavasser Job 33 Form 3api-669728207Pas encore d'évaluation
- Med ReleaseDocument1 pageMed ReleaseMatt SolheimPas encore d'évaluation
- AUH HealthPerfect ApplicationForm en HRDocument4 pagesAUH HealthPerfect ApplicationForm en HRVignesh Kumar HariharPas encore d'évaluation
- Towerview Medical Release FormDocument3 pagesTowerview Medical Release FormCody HudspethPas encore d'évaluation
- Prin. L.N.Welingkar Institute of Management Development and ResearchDocument4 pagesPrin. L.N.Welingkar Institute of Management Development and ResearchKavish JainPas encore d'évaluation
- 2017 Medical Release FormDocument1 page2017 Medical Release FormNafPas encore d'évaluation
- REV - Outpatient Claim Form - AIADocument2 pagesREV - Outpatient Claim Form - AIAYen SylvaniPas encore d'évaluation
- Medical Form & Document ChecklistDocument2 pagesMedical Form & Document Checklistrjadhav0075Pas encore d'évaluation
- Prulife Uk Form PiDocument3 pagesPrulife Uk Form PiPaulie TitoPas encore d'évaluation
- C&a Consent FormsDocument28 pagesC&a Consent Formsjgcj477rh9Pas encore d'évaluation
- Maldives Medical and Dental Council: Application For Registration and Practising LicenseDocument4 pagesMaldives Medical and Dental Council: Application For Registration and Practising LicenseKamran FarooquiPas encore d'évaluation
- Julie Toon Pawley ResumeDocument1 pageJulie Toon Pawley Resumebernardhhi100% (1)
- Footloose Playbill FinalDocument6 pagesFootloose Playbill Finalbernardhhi100% (3)
- Hilton Head Relocation GuideDocument50 pagesHilton Head Relocation GuidebernardhhiPas encore d'évaluation
- Heroes On Horseback Summer 08 NewsletterDocument2 pagesHeroes On Horseback Summer 08 NewsletterbernardhhiPas encore d'évaluation
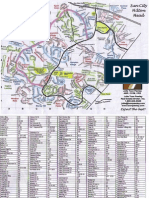
- Sun City Hilton Head Street Map-JTPDocument2 pagesSun City Hilton Head Street Map-JTPbernardhhi100% (3)
- JanFeb 08 WebDocument16 pagesJanFeb 08 WebbernardhhiPas encore d'évaluation
- Ladybird Book - The PolicemanDocument15 pagesLadybird Book - The Policemanbernardhhi91% (11)
- Spring 2008 Continuing-Registration-FormDocument1 pageSpring 2008 Continuing-Registration-FormbernardhhiPas encore d'évaluation
- Summer 2008 Continuing-Registration-FormDocument1 pageSummer 2008 Continuing-Registration-FormbernardhhiPas encore d'évaluation
- HOH Volunteer FormsDocument4 pagesHOH Volunteer FormsbernardhhiPas encore d'évaluation
- Criminal Law Sexual Assault Sexual Intercourse Consent American Medical AssociationDocument7 pagesCriminal Law Sexual Assault Sexual Intercourse Consent American Medical Associationnes_cutyPas encore d'évaluation
- DIGESTED Agrarian Cases 2 3 8 9 10 11Document8 pagesDIGESTED Agrarian Cases 2 3 8 9 10 11ANGIE BERNALPas encore d'évaluation
- IpcDocument22 pagesIpcAmanGupta67% (3)
- Sale of Land 1Document43 pagesSale of Land 1Chinonye OkpoPas encore d'évaluation
- Protection of Tenants (Business Premises) in ZambiaDocument23 pagesProtection of Tenants (Business Premises) in ZambiaAngel MoongaPas encore d'évaluation
- CHA 3 Business LawDocument49 pagesCHA 3 Business LawEbsa AdemePas encore d'évaluation
- Mootcourt Memorial PetitionerDocument15 pagesMootcourt Memorial PetitionerDilip KumarPas encore d'évaluation
- Stambovsky V AckleyDocument4 pagesStambovsky V AckleyKasem AhmedPas encore d'évaluation
- Compiled Conveyancing Work CompletedDocument9 pagesCompiled Conveyancing Work Completedmuenifaith5489Pas encore d'évaluation
- Contract of Indemnity and GuaranteeDocument10 pagesContract of Indemnity and Guaranteecommercewaale1Pas encore d'évaluation
- DR SamuelaDocument2 pagesDR SamuelaMuanchhana MizoPas encore d'évaluation
- L01 Essentials of ContractDocument55 pagesL01 Essentials of ContractRaniya ShoukPas encore d'évaluation
- Contract LawDocument14 pagesContract LawNinad SharmaPas encore d'évaluation
- Qui vs. Court of AppealsDocument9 pagesQui vs. Court of AppealsRheacel LojoPas encore d'évaluation
- Arrangement For The Discussions in Equity and Trusts LLB 2 Stream CDocument7 pagesArrangement For The Discussions in Equity and Trusts LLB 2 Stream CKamugisha JshPas encore d'évaluation
- Contracting and Contract Law - Nilima BhadbhadeDocument102 pagesContracting and Contract Law - Nilima BhadbhadeAngadKamathPas encore d'évaluation
- (Activity 1-4 in Buslaw) Atenta, Alexis Joemel M.Document7 pages(Activity 1-4 in Buslaw) Atenta, Alexis Joemel M.Dashiell Robert ParrPas encore d'évaluation
- Spa:Beauty Lux. Treatments-Hotel Rental Agreement.Document5 pagesSpa:Beauty Lux. Treatments-Hotel Rental Agreement.RenosPas encore d'évaluation
- Data Privacy ManualDocument32 pagesData Privacy ManualBL Trinidad100% (1)
- F4 Breach of Contract and Remedies NotesDocument5 pagesF4 Breach of Contract and Remedies NoteskalinovskayaPas encore d'évaluation
- GMC Guidance For Doctors Confidentiality Patients Fitness To Drive and Reporting Concer 70063275Document3 pagesGMC Guidance For Doctors Confidentiality Patients Fitness To Drive and Reporting Concer 70063275PLAB PREPPas encore d'évaluation
- Addendum To The Franchise Agreement Royalty Fee and Marketing FeeDocument3 pagesAddendum To The Franchise Agreement Royalty Fee and Marketing FeeSUNCREST GAS CORPORATION COMPLIANCE0% (1)
- Contracts Succinct OutlineDocument21 pagesContracts Succinct OutlineAmanda100% (1)
- Vehicle Purchase Agreement 09Document3 pagesVehicle Purchase Agreement 09JF BatucalPas encore d'évaluation
- Unit-2 The Sale of Goods Act 1930Document15 pagesUnit-2 The Sale of Goods Act 1930angelinstanley2003Pas encore d'évaluation
- Consent Token Green PaperDocument13 pagesConsent Token Green PaperConsent TokenPas encore d'évaluation
- Define Contract Under Islamic Law and ItDocument6 pagesDefine Contract Under Islamic Law and ItShabir AhmadPas encore d'évaluation
- An Inchmaree Clause Is A Provision Common in Maritime Insurance Policies That Cover A Ship's Loss or Damage Due To Reasons Such AsDocument5 pagesAn Inchmaree Clause Is A Provision Common in Maritime Insurance Policies That Cover A Ship's Loss or Damage Due To Reasons Such AsSudhendra SoniPas encore d'évaluation
- Petitioner Respondent: Erminda F. Florentino, - Supervalue, Inc.Document10 pagesPetitioner Respondent: Erminda F. Florentino, - Supervalue, Inc.Nicorobin RobinPas encore d'évaluation
- Land Law, Chapter 5Document40 pagesLand Law, Chapter 5khaing zinPas encore d'évaluation