Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Response To Color: Literature Review With Cross-Cultural Marketing PerspectiveDocument8 pagesResponse To Color: Literature Review With Cross-Cultural Marketing Perspectivexaxif8265100% (1)
- Expressing Emotion in Interpersonal InteractionsDocument5 pagesExpressing Emotion in Interpersonal InteractionsAnish PandaPas encore d'évaluation
- Running Head: Professional Development Workshop 1Document27 pagesRunning Head: Professional Development Workshop 1Graham HerrickPas encore d'évaluation
- Will You, As The Human Resource Department Head, Accept The Boss' Will You, As The Human Resource Department Head, Accept The Boss'Document2 pagesWill You, As The Human Resource Department Head, Accept The Boss' Will You, As The Human Resource Department Head, Accept The Boss'marichu apiladoPas encore d'évaluation
- Theorist Theory Implication To Education: Arthur Jensen Theory of IntelligenceDocument30 pagesTheorist Theory Implication To Education: Arthur Jensen Theory of IntelligenceNORY MAE ESCABARTE100% (1)
- The Three Faces of DisciplineDocument4 pagesThe Three Faces of DisciplineAna MurtaPas encore d'évaluation
- Conducting - Action ResearchDocument8 pagesConducting - Action ResearchCossette Rilloraza-MercadoPas encore d'évaluation
- Language Acquisition Myths & RealitiesDocument50 pagesLanguage Acquisition Myths & RealitiesadeelsiddiquepsoPas encore d'évaluation
- Selecting Instructional MediaDocument4 pagesSelecting Instructional Mediaanon_837880857Pas encore d'évaluation
- Teacher Observation ScheduleDocument6 pagesTeacher Observation ScheduleLirioFloresPas encore d'évaluation
- 15 Child PsychologyDocument46 pages15 Child PsychologyVesley B Robin100% (2)
- Lesson 3: Moral Courage: Part 2: THE ACTDocument10 pagesLesson 3: Moral Courage: Part 2: THE ACTHAYLEYPas encore d'évaluation
- Personal Philosophy of Facilitation - PortfolioDocument7 pagesPersonal Philosophy of Facilitation - Portfolioapi-302539316Pas encore d'évaluation
- William BengstonDocument2 pagesWilliam BengstonSever Sava75% (4)
- Homeroom Guidance Mod 1 Grade 12 AnswerDocument19 pagesHomeroom Guidance Mod 1 Grade 12 AnswerMandy Parcero100% (2)
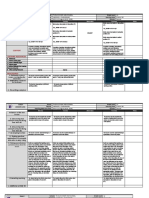
- DLL Smaw and Perdev August 19-23Document7 pagesDLL Smaw and Perdev August 19-23Maricar CarandangPas encore d'évaluation
- Schema/Assimilation/Accommodation: Jean PiagetDocument4 pagesSchema/Assimilation/Accommodation: Jean Piagetciedelle arandaPas encore d'évaluation
- Management Process and Organizational BehaviourDocument9 pagesManagement Process and Organizational BehaviourNageshwar SinghPas encore d'évaluation
- The Best Teaching Strategies Used by TeachersDocument11 pagesThe Best Teaching Strategies Used by TeachersJam JamPas encore d'évaluation
- Change Blindness in The Real WorldDocument3 pagesChange Blindness in The Real WorldKevin GaoPas encore d'évaluation
- CW Marksheet and Cover TemplateDocument3 pagesCW Marksheet and Cover Templatej0r3lmPas encore d'évaluation
- 15142800Document16 pages15142800Sanjeev PradhanPas encore d'évaluation
- HELLER, Valerie - Sexual Liberalism and Survivors of Sexual Abuse PDFDocument5 pagesHELLER, Valerie - Sexual Liberalism and Survivors of Sexual Abuse PDFCarol MariniPas encore d'évaluation
- Rare Me Jaden PintoDocument8 pagesRare Me Jaden PintohemantPas encore d'évaluation
- Seton Hill University Lesson Plan Template: Name Subject Grade Level Date/DurationDocument4 pagesSeton Hill University Lesson Plan Template: Name Subject Grade Level Date/Durationapi-339850286Pas encore d'évaluation
- FS 1 Episode 3Document6 pagesFS 1 Episode 3Princess Ann Pelandas67% (3)
- Oral Communication Module 6Document23 pagesOral Communication Module 6JamRey Vlogs100% (1)
- Chap - 6 RMUPDocument6 pagesChap - 6 RMUPBASHAR AliPas encore d'évaluation
- Love and Mental Health: IntimacyDocument2 pagesLove and Mental Health: IntimacyasdasdasdjdsdPas encore d'évaluation
- Bureaucratic Structure and PersonalityDocument14 pagesBureaucratic Structure and Personalityptdwnhro100% (1)