Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- 10 Historical Speeches Nobody Ever HeardDocument20 pages10 Historical Speeches Nobody Ever HeardSumit Roy100% (1)
- Human Reproductive SystemDocument4 pagesHuman Reproductive SystemGoal Digger Squad VlogPas encore d'évaluation
- Sample SheetDocument3 pagesSample SheetHamdy GabalPas encore d'évaluation
- 00008Document62 pages00008Fernandez-De Ala NicaPas encore d'évaluation
- Science 10: Quarter 3 Module 2 Week 2Document4 pagesScience 10: Quarter 3 Module 2 Week 2Adrian Orrick Capiral80% (5)
- CC, HPV & HPV VaccineDocument16 pagesCC, HPV & HPV VaccineBalqis BaslemanPas encore d'évaluation
- Nursing Seminar 1 SAS Session 4Document8 pagesNursing Seminar 1 SAS Session 4ZiaPas encore d'évaluation
- Gynecological and Obstetrics InstrumentsDocument61 pagesGynecological and Obstetrics InstrumentsRaja33% (3)
- Panduan Tata Laksana Lesi Pra Kanker ServiksDocument76 pagesPanduan Tata Laksana Lesi Pra Kanker ServiksHandy PutraPas encore d'évaluation
- Micro TeachingDocument6 pagesMicro Teachingkawaljitkang100% (1)
- Nightingales - Philips Healthcare Tie UpDocument3 pagesNightingales - Philips Healthcare Tie UpSumit RoyPas encore d'évaluation
- TRAI Data Till 31st March, 2014Document19 pagesTRAI Data Till 31st March, 2014Tamanna Bavishi ShahPas encore d'évaluation
- World Health Days 2014: JanuaryDocument2 pagesWorld Health Days 2014: JanuaryIvy Jorene Roman RodriguezPas encore d'évaluation
- Wereldleiders Op TwitterDocument24 pagesWereldleiders Op TwitterHerman CouwenberghPas encore d'évaluation
- Hepatitis A eDocument1 pageHepatitis A eSumit RoyPas encore d'évaluation
- The State of Mobile Advertising in Emerging Countries TLS EmergingMarketsDocument8 pagesThe State of Mobile Advertising in Emerging Countries TLS EmergingMarketsSumit RoyPas encore d'évaluation
- NokiaDocument1 pageNokiaSumit RoyPas encore d'évaluation
- Hepatitis A eDocument1 pageHepatitis A eSumit RoyPas encore d'évaluation
- Global Top 100 Most Valueable Brands Brandz2014 - Infographic PDFDocument1 pageGlobal Top 100 Most Valueable Brands Brandz2014 - Infographic PDFSumit RoyPas encore d'évaluation
- Risk Factors From Hepatitis BCDDocument1 pageRisk Factors From Hepatitis BCDSumit RoyPas encore d'évaluation
- The State of Airline Marketing Airlinetrends Simpliflying April2013Document21 pagesThe State of Airline Marketing Airlinetrends Simpliflying April2013Sumit RoyPas encore d'évaluation
- Calendário de Jogos Do Mundial de Futebol-Brasil 2014Document0 pageCalendário de Jogos Do Mundial de Futebol-Brasil 2014Miguel RodriguesPas encore d'évaluation
- Mobile Advertising Research Trends and InsightsDocument15 pagesMobile Advertising Research Trends and InsightsSumit RoyPas encore d'évaluation
- The State of Maternal Health, D Nutrition in Asia " World Vision DataDocument4 pagesThe State of Maternal Health, D Nutrition in Asia " World Vision DataSumit RoyPas encore d'évaluation
- Mediamind Comscore Research Dwelling On EntertainmentDocument20 pagesMediamind Comscore Research Dwelling On EntertainmentSumit RoyPas encore d'évaluation
- World Health Statisitics FullDocument180 pagesWorld Health Statisitics FullClarice SalidoPas encore d'évaluation
- Gender and Social Networking Activity :facebook Vs OthersDocument18 pagesGender and Social Networking Activity :facebook Vs OthersSumit RoyPas encore d'évaluation
- FINAL - Mobile Advertising DeckDocument73 pagesFINAL - Mobile Advertising DecksumitkroyPas encore d'évaluation
- MGI China E-Tailing Executive Summary March 2013Document18 pagesMGI China E-Tailing Executive Summary March 2013Sumit RoyPas encore d'évaluation
- Calendar 14Document57 pagesCalendar 14Hanan AhmedPas encore d'évaluation
- 2014 Bill and Melinda Gates Foundation Report On Global PovertyDocument28 pages2014 Bill and Melinda Gates Foundation Report On Global PovertySumit RoyPas encore d'évaluation
- The Evolution of Digital Advertising 3.0: Adobe Research InsightsDocument1 pageThe Evolution of Digital Advertising 3.0: Adobe Research InsightsSumit RoyPas encore d'évaluation
- The 5 Free Alternatives To Microsoft WordDocument60 pagesThe 5 Free Alternatives To Microsoft WordSumit RoyPas encore d'évaluation
- The 5 Free Alternatives To Microsoft WordDocument60 pagesThe 5 Free Alternatives To Microsoft WordSumit RoyPas encore d'évaluation
- CEO Survey On Hiring, Profitability and PeopleDocument36 pagesCEO Survey On Hiring, Profitability and PeopleSumit RoyPas encore d'évaluation
- CVD Atlas 16 Death From Stroke PDFDocument1 pageCVD Atlas 16 Death From Stroke PDFRisti KhafidahPas encore d'évaluation
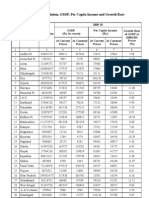
- Statewise GSDP PCI and G.RDocument3 pagesStatewise GSDP PCI and G.RArchit SingalPas encore d'évaluation
- India InfographicsDocument3 pagesIndia InfographicsSumit RoyPas encore d'évaluation
- Dysfunctional Uterine BleedingDocument6 pagesDysfunctional Uterine Bleedingboorai^_^Pas encore d'évaluation
- Complications of PregnancyDocument33 pagesComplications of PregnancyMilagros Maglasang100% (1)
- Female Reproductive Tract AbnormalitiesDocument1 pageFemale Reproductive Tract AbnormalitiesPreethi ShivanandPas encore d'évaluation
- Grade 10 Reproductive HealthDocument26 pagesGrade 10 Reproductive HealthMissy BanguisPas encore d'évaluation
- Treating Endometriosis with Chinese MedicineDocument8 pagesTreating Endometriosis with Chinese Medicineitsik12886Pas encore d'évaluation
- GYN 讀書報告Document67 pagesGYN 讀書報告Chia-Yuan ChenPas encore d'évaluation
- Syarif Taufik's Schedule (1 Session)Document10 pagesSyarif Taufik's Schedule (1 Session)imamsantos1191Pas encore d'évaluation
- Long Quiz 10Document3 pagesLong Quiz 10Jessie GainsanPas encore d'évaluation
- Science 10Document2 pagesScience 10Trisha Camille Macario100% (2)
- Symptoms of Ovarian CancerDocument3 pagesSymptoms of Ovarian Cancerwwe_jhoPas encore d'évaluation
- Case StudyDocument26 pagesCase StudyGrace Orencia100% (1)
- Arbour2013 HypoplasiaDocument5 pagesArbour2013 HypoplasiaCarolina GomezPas encore d'évaluation
- Feeding of Healthy Newborn BabiesDocument37 pagesFeeding of Healthy Newborn BabiesSulfie HarsPas encore d'évaluation
- M.S. Obstetrics & Gynaecology 2020Document32 pagesM.S. Obstetrics & Gynaecology 2020Dr.Udhayakumar sPas encore d'évaluation
- Hemorrhagic ovarian cyst symptoms, causes, treatmentDocument14 pagesHemorrhagic ovarian cyst symptoms, causes, treatmentNyoman TapayanaPas encore d'évaluation
- Diffun Campus: "Molding Minds, Shaping Future"Document41 pagesDiffun Campus: "Molding Minds, Shaping Future"Mary Joy BernasolPas encore d'évaluation
- A Case Report - Ayurvedic Management of Pariplutayonivyapada W.S.R To Pelvic Inflammatory DiseaseDocument6 pagesA Case Report - Ayurvedic Management of Pariplutayonivyapada W.S.R To Pelvic Inflammatory DiseaseIJAR JOURNALPas encore d'évaluation
- Biology AssignmentDocument21 pagesBiology AssignmentKenardPas encore d'évaluation
- Kebersihan Organ Reproduksi Pada Perempuan Pedesaan Di Kelurahan Polaman Kecamatan Mijen SemarangDocument11 pagesKebersihan Organ Reproduksi Pada Perempuan Pedesaan Di Kelurahan Polaman Kecamatan Mijen SemarangDiella Mirabel AmandaPas encore d'évaluation
- Guide: DR Srinath Rao Presenter:Dr SR Soumya (Materia Medica MD Part-1) 15/12/14Document50 pagesGuide: DR Srinath Rao Presenter:Dr SR Soumya (Materia Medica MD Part-1) 15/12/14Krishna Veni100% (2)
- Genital ProlapseDocument40 pagesGenital ProlapseDIPENDRA KUMAR KUSHAWAHAPas encore d'évaluation