Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Names of Allah and Their ReflectionsDocument98 pagesThe Names of Allah and Their ReflectionsSuleyman HldPas encore d'évaluation
- Ashfaque Ahmed-The SAP Materials Management Handbook-Auerbach Publications, CRC Press (2014)Document36 pagesAshfaque Ahmed-The SAP Materials Management Handbook-Auerbach Publications, CRC Press (2014)surajnayak77Pas encore d'évaluation
- Pilar Cyst With CrystalsDocument2 pagesPilar Cyst With CrystalsDeba P SarmaPas encore d'évaluation
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocument6 pagesAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaPas encore d'évaluation
- Acantholytic Dermatosis With DyskeratosisDocument11 pagesAcantholytic Dermatosis With DyskeratosisDeba P SarmaPas encore d'évaluation
- Accessory TragusDocument3 pagesAccessory TragusDeba P SarmaPas encore d'évaluation
- Acantholytic Bullous DiseaseDocument4 pagesAcantholytic Bullous DiseaseDeba P SarmaPas encore d'évaluation
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Document3 pagesAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaPas encore d'évaluation
- Acantholytic Actinic KeratosisDocument4 pagesAcantholytic Actinic KeratosisDeba P SarmaPas encore d'évaluation
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocument7 pagesXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaPas encore d'évaluation
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Document6 pagesBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaPas encore d'évaluation
- Results of Search in Google Scholar On 'Deba P Sarma'Document28 pagesResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaPas encore d'évaluation
- Verrucous Carcinoma of The Foot, M 63, Left FootDocument8 pagesVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Acantholytic Acanthoma. M 60, ScrotumDocument8 pagesAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaPas encore d'évaluation
- Xanthogranuloma, M 30, Right ElbowDocument4 pagesXanthogranuloma, M 30, Right ElbowDeba P SarmaPas encore d'évaluation
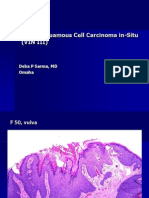
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocument6 pagesVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaPas encore d'évaluation
- Xanthogranuloma PPT DSDocument9 pagesXanthogranuloma PPT DSDeba P SarmaPas encore d'évaluation
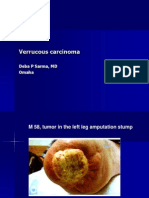
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocument7 pagesVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaPas encore d'évaluation
- Verrucous Epidermal Nevus. F 43, ScalpDocument4 pagesVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaPas encore d'évaluation
- Verruca Vulgaris., M 22.,PPTDocument2 pagesVerruca Vulgaris., M 22.,PPTDeba P SarmaPas encore d'évaluation
- FRQ Vocabulary ReviewDocument1 pageFRQ Vocabulary ReviewDrew AbbottPas encore d'évaluation
- Solutions For Tutorial Exercises Association Rule Mining.: Exercise 1. AprioriDocument5 pagesSolutions For Tutorial Exercises Association Rule Mining.: Exercise 1. AprioriMarkib Singh AdawitahkPas encore d'évaluation
- Cascade Configuration Tool: Installation and Operations ManualDocument22 pagesCascade Configuration Tool: Installation and Operations ManualAndrés GarciaPas encore d'évaluation
- Cover PageDocument10 pagesCover PageAvijit GhoshPas encore d'évaluation
- Et Iso 12543 4 2011Document16 pagesEt Iso 12543 4 2011freddyguzman3471Pas encore d'évaluation
- House Staff OrderDocument2 pagesHouse Staff OrderTarikPas encore d'évaluation
- Goal SettingDocument11 pagesGoal Settingraul_mahadikPas encore d'évaluation
- A Technical Report ON Centre of Pressure ONA Plane Surface ExperimentDocument13 pagesA Technical Report ON Centre of Pressure ONA Plane Surface ExperimentVictor OwolekePas encore d'évaluation
- Device InfoDocument3 pagesDevice InfoGrig TeoPas encore d'évaluation
- EUROJAM Diary3Document4 pagesEUROJAM Diary3Susan BakerPas encore d'évaluation
- HH220i - JAN 11Document1 pageHH220i - JAN 11Achmad GazaliPas encore d'évaluation
- Cyanocobalamin Injection Clinical Pharmacology Drug MonographDocument36 pagesCyanocobalamin Injection Clinical Pharmacology Drug MonographLaureyPas encore d'évaluation
- AA1 Adventure Anthology One r14Document85 pagesAA1 Adventure Anthology One r14dachda100% (1)
- Chapter 34 Esip For FinalDocument35 pagesChapter 34 Esip For FinalJeaniel BorlingPas encore d'évaluation
- LEARNING ACTIVITY SHEET in Oral CommDocument4 pagesLEARNING ACTIVITY SHEET in Oral CommTinTin100% (1)
- FacebookDocument2 pagesFacebookAbhijeet SingarePas encore d'évaluation
- Assignment On Unstable or Astatic Gravimeters and Marine Gravity SurveyDocument9 pagesAssignment On Unstable or Astatic Gravimeters and Marine Gravity Surveyraian islam100% (1)
- 12.3 What Is The Nomenclature System For CFCS/HCFCS/HFCS? (Chemistry)Document3 pages12.3 What Is The Nomenclature System For CFCS/HCFCS/HFCS? (Chemistry)Riska IndriyaniPas encore d'évaluation
- Factsheet AMRT 2023 01Document4 pagesFactsheet AMRT 2023 01arsyil1453Pas encore d'évaluation
- Cesars WayDocument20 pagesCesars WayToni TursićPas encore d'évaluation
- AnnexIIRecommendationsbyHOTCCommittee06 11 18Document6 pagesAnnexIIRecommendationsbyHOTCCommittee06 11 18Bilal AbbasPas encore d'évaluation
- Fluid Mechanics HydraulicsDocument420 pagesFluid Mechanics Hydraulicsanonymousdi3noPas encore d'évaluation
- 8 TH Linear Equations DBDocument1 page8 TH Linear Equations DBParth GoyalPas encore d'évaluation
- IO5 Future Skills Foresight 2030 ReportDocument96 pagesIO5 Future Skills Foresight 2030 ReportjuliavallePas encore d'évaluation
- Self-Actualization in Robert Luketic'S: Legally Blonde: A HumanisticDocument10 pagesSelf-Actualization in Robert Luketic'S: Legally Blonde: A HumanisticAyeshia FréyPas encore d'évaluation
- Decs vs. San DiegoDocument7 pagesDecs vs. San Diegochini17100% (2)
- High School Physics Rutherford Atom Lesson 27Document4 pagesHigh School Physics Rutherford Atom Lesson 27John JohnsonPas encore d'évaluation
- Malnutrition Case StudyDocument3 pagesMalnutrition Case Studyapi-622273373Pas encore d'évaluation