Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
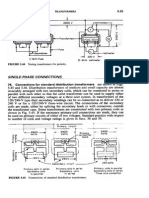
- Transformers ConnectionsDocument6 pagesTransformers Connectionsgeorgel1980Pas encore d'évaluation
- Uppercut MagazineDocument12 pagesUppercut MagazineChris Finn100% (1)
- 2nd Term Study Guide 4th Grade Feb 2024 Cambridge ObjectivesDocument8 pages2nd Term Study Guide 4th Grade Feb 2024 Cambridge Objectivessofi.cardenas1968Pas encore d'évaluation
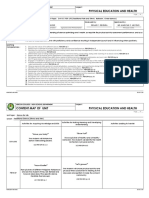
- Content Map PE & Health 12Document12 pagesContent Map PE & Health 12RIZZA MEA DOLOSOPas encore d'évaluation
- Cataloge ICARDocument66 pagesCataloge ICARAgoess Oetomo100% (1)
- Jinko 570 Mono Facial Jkm570m-7rl4-VDocument2 pagesJinko 570 Mono Facial Jkm570m-7rl4-VShahneela AnsariPas encore d'évaluation
- Baxshin LABORATORY: Diagnostic Test and AnalysisDocument1 pageBaxshin LABORATORY: Diagnostic Test and AnalysisJabary HassanPas encore d'évaluation
- Hema Lec HematopoiesisDocument8 pagesHema Lec HematopoiesisWayne ErumaPas encore d'évaluation
- EE2401 Power System Operation and ControlDocument93 pagesEE2401 Power System Operation and ControlPrasanth GovindarajPas encore d'évaluation
- Nursing Management of Anti Fungal DrugsDocument25 pagesNursing Management of Anti Fungal DrugsJennyDaniel100% (1)
- Learning Guide No 5Document19 pagesLearning Guide No 5Menal JemalPas encore d'évaluation
- Solar Powered Water Pumping System PDFDocument46 pagesSolar Powered Water Pumping System PDFVijay Nishad100% (1)
- Plastic As Soil StabilizerDocument28 pagesPlastic As Soil StabilizerKhald Adel KhaldPas encore d'évaluation
- Full Carrino Plaza Brochure and Application (General)Document8 pagesFull Carrino Plaza Brochure and Application (General)tanis581Pas encore d'évaluation
- Top 6 Beginner Work Out MistakesDocument4 pagesTop 6 Beginner Work Out MistakesMARYAM GULPas encore d'évaluation
- The Aging Brain: Course GuidebookDocument126 pagesThe Aging Brain: Course GuidebookIsabel Cristina Jaramillo100% (2)
- Transformers: Z Z Z S S Z S SDocument17 pagesTransformers: Z Z Z S S Z S SSreenivasaraoDharmavarapu100% (1)
- R. Nishanth K. VigneswaranDocument20 pagesR. Nishanth K. VigneswaranAbishaTeslinPas encore d'évaluation
- Boli Vertebro MedulareDocument12 pagesBoli Vertebro MedulareHalit DianaPas encore d'évaluation
- AACO 7th Aviation Fuel Forum: AttendanceDocument3 pagesAACO 7th Aviation Fuel Forum: AttendanceJigisha Vasa0% (1)
- Practice Test For Exam 3 Name: Miguel Vivas Score: - /10Document2 pagesPractice Test For Exam 3 Name: Miguel Vivas Score: - /10MIGUEL ANGELPas encore d'évaluation
- Indirect Current Control of LCL Based Shunt Active Power FilterDocument10 pagesIndirect Current Control of LCL Based Shunt Active Power FilterArsham5033Pas encore d'évaluation
- Celltac MEK 6500Document3 pagesCelltac MEK 6500RiduanPas encore d'évaluation
- OphthalmoplegiaDocument5 pagesOphthalmoplegiaPatricia Feliani SitohangPas encore d'évaluation
- Usp 1078 Good Manufacturing Practices For Bulk Pharmaceutical Excipients PDFDocument13 pagesUsp 1078 Good Manufacturing Practices For Bulk Pharmaceutical Excipients PDFMayson BaliPas encore d'évaluation
- Iso 15011-2-2009Document26 pagesIso 15011-2-2009marcosPas encore d'évaluation
- Photosynthesis PastPaper QuestionsDocument24 pagesPhotosynthesis PastPaper QuestionsEva SugarPas encore d'évaluation
- Oral Rehydration SolutionDocument22 pagesOral Rehydration SolutionAlkaPas encore d'évaluation
- Theories of Learning and Learning MetaphorsDocument4 pagesTheories of Learning and Learning MetaphorsTrisha Mei Nagal50% (2)
- Unit Two The Health Benefits of Physical ActivityDocument10 pagesUnit Two The Health Benefits of Physical ActivityYoseph DefaruPas encore d'évaluation