Vous aimerez peut-être aussi
- PAIN AssessmentDocument63 pagesPAIN Assessmentgyds_17100% (2)
- Pain ManagementDocument49 pagesPain ManagementQasim ChacharPas encore d'évaluation
- Comfort and Pain ManagementDocument75 pagesComfort and Pain ManagementBeverly Lavilla100% (1)
- Understanding Pain Concepts and TreatmentDocument46 pagesUnderstanding Pain Concepts and TreatmentwokorowPas encore d'évaluation
- نسخة Lecture - PAIN Assessment & ManagementDocument52 pagesنسخة Lecture - PAIN Assessment & Managementjsoal100% (1)
- Pain Physiology Pathways Mechanisms ClassificationDocument71 pagesPain Physiology Pathways Mechanisms Classificationkeerthi_keshapagaPas encore d'évaluation
- Pain Management For NursesDocument42 pagesPain Management For Nursesblacknurse100% (1)
- Interventional Pain: A Step-by-Step Guide for the FIPP ExamD'EverandInterventional Pain: A Step-by-Step Guide for the FIPP ExamAgnes R. StogiczaPas encore d'évaluation
- Minimally Invasive Surgery for Chronic Pain Management: An Evidence-Based ApproachD'EverandMinimally Invasive Surgery for Chronic Pain Management: An Evidence-Based ApproachGiorgio PietramaggioriPas encore d'évaluation
- Movements and Orthopedic Tests: quick, easy, and reliableD'EverandMovements and Orthopedic Tests: quick, easy, and reliablePas encore d'évaluation
- Trochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandTrochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Pain ManagementDocument175 pagesPain ManagementGusni FitriPas encore d'évaluation
- PainDocument35 pagesPainixora n100% (1)
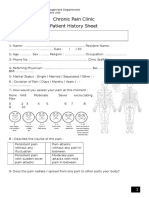
- Chronic Pain Clinic Patient History SheetDocument4 pagesChronic Pain Clinic Patient History SheetBelal N. MahfouzPas encore d'évaluation
- DR - Muhammad Aasam Maan: Consultant Pain SpecialistDocument23 pagesDR - Muhammad Aasam Maan: Consultant Pain SpecialistMuhammad Aasim MaanPas encore d'évaluation
- The stellate ganglion is located anterior to the transverse processes of C7 and T1 vertebraeDocument287 pagesThe stellate ganglion is located anterior to the transverse processes of C7 and T1 vertebraeSAJID ALIPas encore d'évaluation
- Cervical Spine DisorderDocument9 pagesCervical Spine DisorderANDRE MAPas encore d'évaluation
- Assessment Management of PainDocument104 pagesAssessment Management of PainCharles B. LópezPas encore d'évaluation
- Pain AssessmentDocument11 pagesPain AssessmentJenjen Cortey100% (1)
- PAIN and Pain Management PDFDocument56 pagesPAIN and Pain Management PDFcj bariasPas encore d'évaluation
- Pain ManagementDocument175 pagesPain ManagementBobby Noel Cerro Jr100% (4)
- PainDocument230 pagesPainAnonymous uGbcVSJTDg100% (8)
- Pain SecretsDocument790 pagesPain SecretsAaron Jones100% (7)
- PAIN MANAGEMENT GUIDEDocument51 pagesPAIN MANAGEMENT GUIDEdr Sarvesh B100% (1)
- Complex Regional Pain SyndromeDocument10 pagesComplex Regional Pain SyndromegeejeiPas encore d'évaluation
- Handbook of Pain ManagementDocument730 pagesHandbook of Pain Managementanon_990504998100% (6)
- Final - Pain ManagementDocument18 pagesFinal - Pain ManagementFatma Shnewra100% (1)
- Acute PainDocument348 pagesAcute PainBoge Trca Trcoski100% (3)
- Pain and Pain ManagementDocument22 pagesPain and Pain ManagementChen Li100% (1)
- From Acute To Chronic Back PainDocument607 pagesFrom Acute To Chronic Back PainHugo Falqueto100% (2)
- Good Template To Keep 27 September 2013Document3 pagesGood Template To Keep 27 September 2013anuPas encore d'évaluation
- Minimally invasive lumbar spine decompression guideDocument10 pagesMinimally invasive lumbar spine decompression guidePankaj Vatsa100% (1)
- Pain & PainDocument78 pagesPain & PainChalla_Mallika_4532100% (1)
- Submitted By: Group 74 Submitted To: Mrs. Mary Jeannie PatrimonioDocument30 pagesSubmitted By: Group 74 Submitted To: Mrs. Mary Jeannie Patrimonioanon_89298Pas encore d'évaluation
- Electroconvulsive Therapy: Aban, Katherine Maebelle G. Esguerra, Dianne Carmela RDocument46 pagesElectroconvulsive Therapy: Aban, Katherine Maebelle G. Esguerra, Dianne Carmela REdgar ManoodPas encore d'évaluation
- MCQs in Pain Medicine: Effective Treatments and Red FlagsDocument7 pagesMCQs in Pain Medicine: Effective Treatments and Red FlagsPrav Ganty50% (2)
- Trigeminal NeuralgiaDocument23 pagesTrigeminal Neuralgiaekiferdianto100% (1)
- Anesthesia For Electroconvulsive TherapyDocument28 pagesAnesthesia For Electroconvulsive TherapyLowell RebucalPas encore d'évaluation
- PAIN PATHWAY: THE BODY'S ALARM SYSTEMDocument70 pagesPAIN PATHWAY: THE BODY'S ALARM SYSTEMDr Mirunalini SundaravadiveluPas encore d'évaluation
- PainDocument90 pagesPainmikErlh100% (4)
- 282-Essentials of Pain Management-Nalini Vadivelu Richard D. Urman Roberta L. Hines-0387875786-Sp PDFDocument859 pages282-Essentials of Pain Management-Nalini Vadivelu Richard D. Urman Roberta L. Hines-0387875786-Sp PDFarief-024100% (2)
- ATLAS OF INTERVENTIONAL PAIN MANAGEMENT, 4ed PDFDocument1 164 pagesATLAS OF INTERVENTIONAL PAIN MANAGEMENT, 4ed PDFjesussalvadorsuazaPas encore d'évaluation
- Pain Management CardDocument2 pagesPain Management Cardlrpokhrel50% (2)
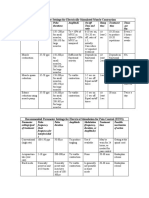
- Parameter Settings for Electrical StimulationDocument3 pagesParameter Settings for Electrical Stimulationpallen100% (5)
- Cardiac Valve Disorders: Etiology, Pathophysiology, Diagnosis and ManagementDocument80 pagesCardiac Valve Disorders: Etiology, Pathophysiology, Diagnosis and ManagementRachilla Arandita SaraswatiPas encore d'évaluation
- Chronic PainDocument269 pagesChronic PainAdrian Anca100% (4)
- Generic (Brand) Name Use Considerations: Table of Selected Medications Used in Pain ManagementDocument4 pagesGeneric (Brand) Name Use Considerations: Table of Selected Medications Used in Pain Managementrifal akbarPas encore d'évaluation
- 24 Top Orthopedic TestsDocument29 pages24 Top Orthopedic TestsDavid Gal100% (1)
- Neurological ExaminationDocument9 pagesNeurological Examinationmohitnet1327Pas encore d'évaluation
- Special Tests of The Spine 1Document33 pagesSpecial Tests of The Spine 1Charles Jefferson Yamogan JiongcoPas encore d'évaluation
- Handbook of Pain Management PDFDocument105 pagesHandbook of Pain Management PDFsatyagraha84Pas encore d'évaluation
- Mixed Pain DR Novi Irawan SPSDocument25 pagesMixed Pain DR Novi Irawan SPSnovi irawanPas encore d'évaluation
- Orthopedics MnemonicsDocument6 pagesOrthopedics MnemonicsTefera LeteboPas encore d'évaluation
- Thoracic PainDocument36 pagesThoracic PainLuciana ThioPas encore d'évaluation
- Chronic Pain Assessment QuestionnaireDocument2 pagesChronic Pain Assessment QuestionnaireHosam Mahmoud100% (1)
- 52 Page PDF PF PPT Neurophysiological Effects of Spinal Manual Therapy in The Upper Extremity - ChuDocument52 pages52 Page PDF PF PPT Neurophysiological Effects of Spinal Manual Therapy in The Upper Extremity - ChuDenise MathrePas encore d'évaluation
- Sleep Disorder Evaluation TemplateDocument2 pagesSleep Disorder Evaluation Templatee-MedTools100% (12)
- Analgesics Chronic PainDocument36 pagesAnalgesics Chronic PainRobMarvinPas encore d'évaluation
- Acute Postoperative Pain Manila Relef.Document134 pagesAcute Postoperative Pain Manila Relef.Muchtar Luthfi100% (1)
- Ojimd Handbook of Acute Pain ManagementDocument338 pagesOjimd Handbook of Acute Pain ManagementVytautas PilelisPas encore d'évaluation
- Test Bank For Therapeutic Modalities 4th EditionDocument5 pagesTest Bank For Therapeutic Modalities 4th EditionBecky Ramirez100% (26)
- Pain Physiology Pathways Mechanisms ClassificationDocument71 pagesPain Physiology Pathways Mechanisms Classificationkeerthi_keshapagaPas encore d'évaluation
- Types of PainDocument1 pageTypes of PainIntan Putri Wirahana ShantyPas encore d'évaluation
- Revisiting The Continuum Model of Tendon PathologyDocument8 pagesRevisiting The Continuum Model of Tendon PathologyDavid DiazPas encore d'évaluation
- Primer: Tension-Type HeadacheDocument21 pagesPrimer: Tension-Type HeadachefiqriPas encore d'évaluation
- Types of PainDocument4 pagesTypes of PainJordi FontPas encore d'évaluation
- Neuropathic Pain MechanismsDocument14 pagesNeuropathic Pain Mechanismsfahri azwarPas encore d'évaluation
- Pain Mechanism: Walton and Torabinejad. Principles and Practice of Endodontics 3Document6 pagesPain Mechanism: Walton and Torabinejad. Principles and Practice of Endodontics 3nilafebryPas encore d'évaluation
- Dental Pain Pathway and MechanismDocument19 pagesDental Pain Pathway and MechanismMsambaruke Mch100% (2)
- (Perspectives in Nursing Management and Care For Older Adults) Gisèle Pickering, Sandra Zwakhalen, Sharon Kaasalainen - Pain Management in Older Adults-Springer International Publishing (2018) PDFDocument142 pages(Perspectives in Nursing Management and Care For Older Adults) Gisèle Pickering, Sandra Zwakhalen, Sharon Kaasalainen - Pain Management in Older Adults-Springer International Publishing (2018) PDFEva Yuliana YulianaPas encore d'évaluation
- Nihms 396443Document12 pagesNihms 396443kickinghorse892Pas encore d'évaluation
- Journal of NeurosurgeryDocument9 pagesJournal of NeurosurgeryYoga Rossi Widya UtamaPas encore d'évaluation
- Acutepainmanagement: Nabil Moussa,, Orrett E. OgleDocument13 pagesAcutepainmanagement: Nabil Moussa,, Orrett E. OgleMahmoud AbouelsoudPas encore d'évaluation
- Pain Is in The Brain HandoutDocument39 pagesPain Is in The Brain Handoutgabitor100% (1)
- Agung HidayatullahDocument58 pagesAgung HidayatullahIta Aprilia SaktiPas encore d'évaluation
- ManualDocument81 pagesManualmumtonagPas encore d'évaluation
- Pain: Current Understanding of Assessment, Management, and TreatmentsDocument101 pagesPain: Current Understanding of Assessment, Management, and TreatmentsNational Pharmaceutical Council100% (8)
- Technical PDFDocument41 pagesTechnical PDFSergio Sandoval100% (3)
- 1 Pain - 2013 - A System of Orthopaedic Medicine Third Edition PDFDocument19 pages1 Pain - 2013 - A System of Orthopaedic Medicine Third Edition PDFMadalina ArtenePas encore d'évaluation
- Assignment Cover Page - PathophysiologyDocument6 pagesAssignment Cover Page - PathophysiologyAnonymous HcjWDGDnPas encore d'évaluation
- Overview of Pain: Classification and Concepts: James Woessner, M.D., PH.DDocument14 pagesOverview of Pain: Classification and Concepts: James Woessner, M.D., PH.DAnonymous S0MyRHPas encore d'évaluation
- Basics of Pain Management: Vanny Le, MD Assistant Professor Department of AnesthesiologyDocument28 pagesBasics of Pain Management: Vanny Le, MD Assistant Professor Department of AnesthesiologyVanny LePas encore d'évaluation
- Patofisiologi Nyeri DasarDocument87 pagesPatofisiologi Nyeri DasarHidayat Bazeher0% (1)
- Lisa Johnson, Ba, SRS, Latg Certification Review Session 2010 Asr Annual Meeting Clearwater Beach, FLDocument33 pagesLisa Johnson, Ba, SRS, Latg Certification Review Session 2010 Asr Annual Meeting Clearwater Beach, FLAnonymous cCMY2pPas encore d'évaluation
- Medsurg Nursing KEY POINTS Lecture Notes Ch1 69Document324 pagesMedsurg Nursing KEY POINTS Lecture Notes Ch1 69jamielyzaPas encore d'évaluation
- Introduction To Pain: MakassarDocument55 pagesIntroduction To Pain: MakassarNizwan ShamPas encore d'évaluation
- Cancer PainDocument52 pagesCancer PainIndraYudhi100% (1)
- Pharmacology of Opioids: Maher Khdour, Msc. PHD Clinical PharmacyDocument66 pagesPharmacology of Opioids: Maher Khdour, Msc. PHD Clinical PharmacyYousef JafarPas encore d'évaluation
- MCQ Pathways9th.IDocument4 pagesMCQ Pathways9th.Iareej alblowi100% (1)