Vous aimerez peut-être aussi
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Flares & VentsDocument29 pagesFlares & VentsSonu Kaka KakaPas encore d'évaluation
- Notes On Peck&Coyle Practical CriticismDocument10 pagesNotes On Peck&Coyle Practical CriticismLily DamePas encore d'évaluation
- 5-2 Sem2 Phys ExamDocument7 pages5-2 Sem2 Phys ExamNayLinPas encore d'évaluation
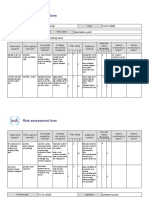
- Risk Assessment Project Iosh - MsDocument2 pagesRisk Assessment Project Iosh - MsSanjeev Kumar75% (32)
- Statistical Mechanics PDFDocument578 pagesStatistical Mechanics PDFraymon6666100% (6)
- 3 Particle Nature of Matter PDFDocument4 pages3 Particle Nature of Matter PDFAtheer AlaniPas encore d'évaluation
- The Effective SpanDocument4 pagesThe Effective SpanMohamed FarahPas encore d'évaluation
- Aqa Econ3 QP Jan12Document8 pagesAqa Econ3 QP Jan12api-247036342Pas encore d'évaluation
- Examination Speaking Assignments Term III - 2021Document2 pagesExamination Speaking Assignments Term III - 2021Khrystyna ShkilniukPas encore d'évaluation
- Commissioning/Troubleshooting: Check List: C B A Yellow Grey Black TBPDocument2 pagesCommissioning/Troubleshooting: Check List: C B A Yellow Grey Black TBPmohamedPas encore d'évaluation
- 0 Act Sunum 2020 NewwDocument58 pages0 Act Sunum 2020 NewwPınar AdsızPas encore d'évaluation
- Instrumentation & Measurement SystemsDocument7 pagesInstrumentation & Measurement SystemsAnkit KumarPas encore d'évaluation
- 365-M - City Bus Route & Timings, Bangalore (BMTC) Map, First & Last BusDocument10 pages365-M - City Bus Route & Timings, Bangalore (BMTC) Map, First & Last BusER Aditya DasPas encore d'évaluation
- Spread of Hinduism To South East Asia by Land and Maritime RoutesDocument36 pagesSpread of Hinduism To South East Asia by Land and Maritime RoutesUday DokrasPas encore d'évaluation
- Lesson 5 African LiteratureDocument3 pagesLesson 5 African LiteratureMiguel CarloPas encore d'évaluation
- Yamaha MG16 PDFDocument2 pagesYamaha MG16 PDFmiskoyu027Pas encore d'évaluation
- Application of Land Suitability AnalysisDocument16 pagesApplication of Land Suitability AnalysisHải Anh Nguyễn100% (1)
- Relay Identification: Example CDG31FF002SACHDocument5 pagesRelay Identification: Example CDG31FF002SACHRohit RanaPas encore d'évaluation
- Manuel D'utilisation Maison AnglaisDocument17 pagesManuel D'utilisation Maison AnglaisVanesssPas encore d'évaluation
- Pakistan PresentationDocument17 pagesPakistan PresentationYaseen Khan100% (1)
- Divine Child International School, Adalaj Revision Worksheet Grade 6, Maths Choose The Correct OptionDocument2 pagesDivine Child International School, Adalaj Revision Worksheet Grade 6, Maths Choose The Correct OptionNatasha VidhaniPas encore d'évaluation
- IoT & WSN - Module 5 - 2018 by Prof - SVDocument43 pagesIoT & WSN - Module 5 - 2018 by Prof - SVVignesh MJ83% (6)
- Unit-4 - Hypothesis TestingDocument24 pagesUnit-4 - Hypothesis TestingMANTHAN JADHAVPas encore d'évaluation
- PRICELIST E Katalogs IVD 06042023 INDOPUTRA - PDF TerbaruDocument6 pagesPRICELIST E Katalogs IVD 06042023 INDOPUTRA - PDF Terbaruseksi sspk sarprasPas encore d'évaluation
- Ycaj CHILLERDocument108 pagesYcaj CHILLERAbhilash Joseph100% (2)
- TNM Sites May 2023Document24 pagesTNM Sites May 2023Joseph ChikusePas encore d'évaluation
- Gayatri Mantras of Several GodDocument10 pagesGayatri Mantras of Several GodAnup KashyapPas encore d'évaluation
- CF1900SS-DF Example Spec - Rev1Document1 pageCF1900SS-DF Example Spec - Rev1parsiti unnesPas encore d'évaluation
- LightsDocument33 pagesLightsEduardo Almeida SilvaPas encore d'évaluation
- Art 16-18Document528 pagesArt 16-18ErudíhenPas encore d'évaluation