Vous aimerez peut-être aussi
- Sirosis HepatisDocument29 pagesSirosis HepatisXaverius da CunhaPas encore d'évaluation
- Aki Et Causa Gastroenteritis Acute and DM Type 2Document26 pagesAki Et Causa Gastroenteritis Acute and DM Type 2Vitya ResanindyaPas encore d'évaluation
- CR Destroyed LungDocument42 pagesCR Destroyed LungAndre Prasetyo MahesyaPas encore d'évaluation
- Tutorial Bu MiniDocument21 pagesTutorial Bu MiniBagus Ayu PurnamasariPas encore d'évaluation
- PR CBD DR LusitoDocument66 pagesPR CBD DR LusitoFebry Hw PratamaPas encore d'évaluation
- GerdDocument23 pagesGerdAin HaririPas encore d'évaluation
- Case ReportDocument22 pagesCase ReportCitra PusvitaliaPas encore d'évaluation
- Acute Nephrotic SyndromeDocument10 pagesAcute Nephrotic SyndromeEvi SilviaPas encore d'évaluation
- Duty Report On Ward 24-06-15Document25 pagesDuty Report On Ward 24-06-15Annisa Rizki Ratih PratiwiPas encore d'évaluation
- Myelodisplastic SyndromeDocument29 pagesMyelodisplastic SyndromeTiara RahmawatiPas encore d'évaluation
- Case CHF, Cap, DM Tipe 2 - Dr. Ruddy, SP - PDDocument34 pagesCase CHF, Cap, DM Tipe 2 - Dr. Ruddy, SP - PDMelisaPas encore d'évaluation
- Presentasi Kasus Dokter Arif Cynthia NataliaDocument26 pagesPresentasi Kasus Dokter Arif Cynthia NataliaIntan SorayaPas encore d'évaluation
- English Case JaundiceDocument38 pagesEnglish Case JaundiceCavin HandokoPas encore d'évaluation
- Morning Report RakaDocument19 pagesMorning Report Rakaraka widhiartaPas encore d'évaluation
- Meig SyndromeDocument42 pagesMeig SyndromeWenny Artha MuliaPas encore d'évaluation
- Case Report 1 - IsKDocument21 pagesCase Report 1 - IsKwulanPas encore d'évaluation
- Edited HP I Fri ConfDocument85 pagesEdited HP I Fri ConfTara Oliveros Dela CruzPas encore d'évaluation
- Imed Case 5Document11 pagesImed Case 5Shakshi RainaPas encore d'évaluation
- Morning Report GEA-15DesDocument12 pagesMorning Report GEA-15DeszakyalfathuPas encore d'évaluation
- Parade Bedah Urology-1Document22 pagesParade Bedah Urology-1Ide Yudis TiyoPas encore d'évaluation
- Case Series CapDocument162 pagesCase Series CapDhruva PatelPas encore d'évaluation
- Final CaseDocument45 pagesFinal Case_carido_Pas encore d'évaluation
- Chronic Obstructive PulmonaryDocument28 pagesChronic Obstructive PulmonaryAyu Sulung NariratriPas encore d'évaluation
- Grand ReportsDocument60 pagesGrand ReportsfilchibuffPas encore d'évaluation
- Group 2: Vaibhav Jain Kaliyannan Kayalvizhi Krishnamoorthy Srinath Kumar EswariDocument35 pagesGroup 2: Vaibhav Jain Kaliyannan Kayalvizhi Krishnamoorthy Srinath Kumar EswariZedd ZorïPas encore d'évaluation
- Morning Report: Name: DM Albert, DM Vira, DM Elvin Konsulen: Dr. Alders, Sp. BDocument18 pagesMorning Report: Name: DM Albert, DM Vira, DM Elvin Konsulen: Dr. Alders, Sp. BElvin DergongPas encore d'évaluation
- Afternoon Report: Monday, May 10 2021 Case From Friday, May 7 2021Document24 pagesAfternoon Report: Monday, May 10 2021 Case From Friday, May 7 2021diahkusumawatiPas encore d'évaluation
- CASE REPORT Dr. Arie Polim, SpOG FinalDocument50 pagesCASE REPORT Dr. Arie Polim, SpOG FinalpriskavkPas encore d'évaluation
- Case Conference Saturday Night Shift, APRIL 6 TH, 2019Document46 pagesCase Conference Saturday Night Shift, APRIL 6 TH, 2019delfiaPas encore d'évaluation
- Oral Revalida Im Cases Dec. 12 and 13 2020Document16 pagesOral Revalida Im Cases Dec. 12 and 13 2020Bea Y. Bas-ongPas encore d'évaluation
- Case Series - CapDocument162 pagesCase Series - CapMichael LinebargerPas encore d'évaluation
- STEMI Whole Anterior Onset 24 Hours Killip I: TIMI Score 6:14Document26 pagesSTEMI Whole Anterior Onset 24 Hours Killip I: TIMI Score 6:14Akbar IskandarPas encore d'évaluation
- Case GNApsDocument47 pagesCase GNApsAndhika Hadi WirawanPas encore d'évaluation
- Duty Report Er 23 07 2015Document25 pagesDuty Report Er 23 07 2015Auditya WidyasariPas encore d'évaluation
- +CBD ANEMIA, ABDOMINAL PAIN DR Saugi - MuznaDocument36 pages+CBD ANEMIA, ABDOMINAL PAIN DR Saugi - MuznaAlmira PratiwiPas encore d'évaluation
- DUTY REPORT Igd Ecy AbeDocument21 pagesDUTY REPORT Igd Ecy AbeAsiah AbdillahPas encore d'évaluation
- "Morning Report": Christian University of IndonesiaDocument12 pages"Morning Report": Christian University of IndonesialettasamudraPas encore d'évaluation
- Pedia WW Patient AmDocument32 pagesPedia WW Patient AmSam Raven AndresPas encore d'évaluation
- Morning Report Tuesday Night Shift, FEBRUARY 12, 2019: Dr. / Dr. / Dr. / Dr. /dr. Dr. Dr. / DRDocument32 pagesMorning Report Tuesday Night Shift, FEBRUARY 12, 2019: Dr. / Dr. / Dr. / Dr. /dr. Dr. Dr. / DRHafizhan MuhammadPas encore d'évaluation
- General Surgery: Saturday, March 20th 2021Document20 pagesGeneral Surgery: Saturday, March 20th 2021ida ayu tungga dewiPas encore d'évaluation
- Pedia PPT1Document52 pagesPedia PPT1Jan Mikhail FrascoPas encore d'évaluation
- Caseeeee Egaaa IrbasssDocument27 pagesCaseeeee Egaaa IrbasssIrbasMantiniSyaifulPas encore d'évaluation
- Case - IUFDDocument5 pagesCase - IUFDMaris Sarline OpenianoPas encore d'évaluation
- 106, Mrs T 36 Hydatiform MoleDocument16 pages106, Mrs T 36 Hydatiform MoleShawn DyerPas encore d'évaluation
- DMDFDocument22 pagesDMDFsujal177402100% (1)
- Morning ReportDocument15 pagesMorning ReportMuh FitrahPas encore d'évaluation
- Case PresentationDocument31 pagesCase PresentationArsalan NadeemPas encore d'évaluation
- Presentation Bedah UmumDocument17 pagesPresentation Bedah Umumida ayu tungga dewiPas encore d'évaluation
- Morning Report: Disusun Oleh: Noermawati DewiDocument38 pagesMorning Report: Disusun Oleh: Noermawati DewidevyPas encore d'évaluation
- Morning Report: Disusun Oleh: Devy Puspo WardoyoDocument36 pagesMorning Report: Disusun Oleh: Devy Puspo WardoyodevyPas encore d'évaluation
- Leptos 2 With Meta AnalysisDocument26 pagesLeptos 2 With Meta AnalysisCms CSUPas encore d'évaluation
- Duty Report 1 June 2016: PPDS On Duty: Dr. Rizki Febriani Putri Coass On Duty: Chaerunisa and VatianaDocument21 pagesDuty Report 1 June 2016: PPDS On Duty: Dr. Rizki Febriani Putri Coass On Duty: Chaerunisa and VatianaRizky GumelarPas encore d'évaluation
- Surgery Department: Case PresentationDocument13 pagesSurgery Department: Case PresentationJayarajan RvjPas encore d'évaluation
- "Morning Report": Department of Internal MedicineDocument12 pages"Morning Report": Department of Internal MedicineAdli NurfakhriPas encore d'évaluation
- MR Dss SanglahDocument19 pagesMR Dss SanglahAnindya AgrasidiPas encore d'évaluation
- Case Based DiscussionDocument9 pagesCase Based DiscussionZigran HakimPas encore d'évaluation
- Case Presentation Febrile FitDocument33 pagesCase Presentation Febrile FitNurul Syazwani RamliPas encore d'évaluation
- Rectal CancerDocument71 pagesRectal CancerGio Balisi100% (2)
- Morning Report: Monday, January 8th, 2018Document17 pagesMorning Report: Monday, January 8th, 2018SyahnasMasterinaPas encore d'évaluation
- Urinary Tract Infection: Mentor DR - SaralaDocument53 pagesUrinary Tract Infection: Mentor DR - SaralaMimi Suhaini SudinPas encore d'évaluation
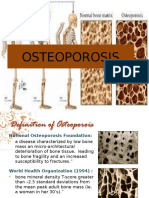
- OsteoporosisDocument13 pagesOsteoporosisMimi Suhaini SudinPas encore d'évaluation
- Case ReportDocument45 pagesCase ReportMimi Suhaini SudinPas encore d'évaluation
- ED Case Discussion - TraumaDocument23 pagesED Case Discussion - TraumaMimi Suhaini SudinPas encore d'évaluation
- Case ReportDocument45 pagesCase ReportMimi Suhaini SudinPas encore d'évaluation
- UTIDocument53 pagesUTIMimi Suhaini SudinPas encore d'évaluation
- Comparison of Ivermectin and Benzyl Benzoate Lotion For ScabiesDocument10 pagesComparison of Ivermectin and Benzyl Benzoate Lotion For ScabiesMimi Suhaini SudinPas encore d'évaluation
- Hyperemesis GravidarumDocument17 pagesHyperemesis GravidarumHo PingPas encore d'évaluation
- By: Mimi Suhaini BT Sudin 030.08.308 Kepaniteraan Ilmu Kandungan Dan Kebidanan RSAL Fakultas Kedokteran TrisaktiDocument11 pagesBy: Mimi Suhaini BT Sudin 030.08.308 Kepaniteraan Ilmu Kandungan Dan Kebidanan RSAL Fakultas Kedokteran TrisaktiMimi Suhaini SudinPas encore d'évaluation
- JournalDocument11 pagesJournalMimi Suhaini SudinPas encore d'évaluation
- Traction & CastingDocument41 pagesTraction & CastingMimi Suhaini SudinPas encore d'évaluation
- EDS EditDocument35 pagesEDS EditMimi Suhaini SudinPas encore d'évaluation
- Dislokasi BahuDocument19 pagesDislokasi BahuShaeima ShamsuddinPas encore d'évaluation
- Dislokasi BahuDocument19 pagesDislokasi BahuShaeima ShamsuddinPas encore d'évaluation
- Kaki DiabetesRSMM 2012Document34 pagesKaki DiabetesRSMM 2012Mimi Suhaini SudinPas encore d'évaluation
- NERVOUS SYSTEM - pptx-2Document39 pagesNERVOUS SYSTEM - pptx-2jeffinjoffiPas encore d'évaluation
- 101 Anti-TPO-V2.3-EN-20130731Document4 pages101 Anti-TPO-V2.3-EN-20130731Iancu Adina FloricicaPas encore d'évaluation
- DevelopmentofocclusionDocument33 pagesDevelopmentofocclusionDeepak NarayanPas encore d'évaluation
- A&P Principles of Microbiology and Human Disease (Nursing) - PowerPointDocument47 pagesA&P Principles of Microbiology and Human Disease (Nursing) - PowerPointLinsey Bowen100% (2)
- Ent SpottersDocument18 pagesEnt SpottersJithin Gopal100% (1)
- OSCE Checklist Newborn Baby Assessment NIPEDocument3 pagesOSCE Checklist Newborn Baby Assessment NIPETauqeer Ahmed0% (1)
- Medical Examination Form For KASDocument15 pagesMedical Examination Form For KASMj PayalPas encore d'évaluation
- IV Fluid TherapyDocument28 pagesIV Fluid TherapyJacinta MaryPas encore d'évaluation
- Dairy Farmers Training ManualDocument98 pagesDairy Farmers Training ManualGrowel Agrovet Private Limited.100% (1)
- 10 Anatomy of The Thoracic Aorta and of Its BranchesDocument9 pages10 Anatomy of The Thoracic Aorta and of Its BranchesStefanPas encore d'évaluation
- Vegan - The Healthiest DietDocument32 pagesVegan - The Healthiest DietVegan Future100% (4)
- 7.digestive SystemDocument29 pages7.digestive SystemMai Z HaniyaPas encore d'évaluation
- Physiology of Muscle Contraction and Control of MovementDocument69 pagesPhysiology of Muscle Contraction and Control of MovementMakmunNawil100% (1)
- Topic Test: Oxfordaqa International Gcse Biology 9201Document26 pagesTopic Test: Oxfordaqa International Gcse Biology 9201Novanolo Christovori ZebuaPas encore d'évaluation
- LPL - PSC Rohini (DC Chowk) Shop No. 27, Ground Floor, SG Mall, Sect or - 9, DC Chowk, Rohini New Delhi - 110 DelhiDocument2 pagesLPL - PSC Rohini (DC Chowk) Shop No. 27, Ground Floor, SG Mall, Sect or - 9, DC Chowk, Rohini New Delhi - 110 DelhiSaurabh GuptaPas encore d'évaluation
- Anterior Cross Bites in Primary Mixed Dentition PedoDocument32 pagesAnterior Cross Bites in Primary Mixed Dentition PedoFourthMolar.comPas encore d'évaluation
- Microbiology ReviewerDocument3 pagesMicrobiology ReviewerWendy Escalante100% (6)
- Plr9 and Procedure For Lab Activity 9 MicparaDocument3 pagesPlr9 and Procedure For Lab Activity 9 MicparaLance sorianoPas encore d'évaluation
- Lecture Notes - MEDICAL PARASITOLOGYDocument12 pagesLecture Notes - MEDICAL PARASITOLOGYAngelica Marzo67% (3)
- 2018 - The Growth and Body Composition of AnimalDocument5 pages2018 - The Growth and Body Composition of AnimalZaheer HussainPas encore d'évaluation
- Us English 2024Document11 pagesUs English 2024yuniati668Pas encore d'évaluation
- Dutton Chapter 24 The Temporomandibular JointDocument47 pagesDutton Chapter 24 The Temporomandibular JointdralismPas encore d'évaluation
- Human Biological and Cultural EvolutionDocument51 pagesHuman Biological and Cultural Evolutionmichael0202Pas encore d'évaluation
- Vaccinations For ChildrenDocument6 pagesVaccinations For Childrenapi-358040298Pas encore d'évaluation
- WDJ 0709Document24 pagesWDJ 0709健康生活園Healthy Life GardenPas encore d'évaluation
- Histology SyllabusDocument32 pagesHistology SyllabusAdrianAddieNovioDeJesusPas encore d'évaluation
- Robbins Pathology - Chapter 6 TransDocument31 pagesRobbins Pathology - Chapter 6 Transnath nathPas encore d'évaluation
- HeartDocument72 pagesHeartfyzanfroshie100% (1)
- Clinical ChemistryDocument14 pagesClinical ChemistryMio Vida100% (1)
- Fisier 2 Urgente Digestive EtcDocument136 pagesFisier 2 Urgente Digestive EtcDaniela PopPas encore d'évaluation