Vous aimerez peut-être aussi
- Clinical Embriology and Anatomy of Gi Tract Part1Document44 pagesClinical Embriology and Anatomy of Gi Tract Part1trianaamalia100% (1)
- GIT EmbryologyDocument39 pagesGIT Embryologyqnz78swpjmPas encore d'évaluation
- Duodenum and PancreaslectureDocument35 pagesDuodenum and PancreaslectureChigozie GeraldPas encore d'évaluation
- DIgestive System EmbDocument85 pagesDIgestive System EmbDanish GujjarPas encore d'évaluation
- Abdominal CavityDocument78 pagesAbdominal Cavitytanishapatel1005Pas encore d'évaluation
- Anatomy of GALL BLADDER PANCREAS 2016Document32 pagesAnatomy of GALL BLADDER PANCREAS 2016Omar Ali AyoubkhanPas encore d'évaluation
- Embryology of the Gastrointestinal TractDocument58 pagesEmbryology of the Gastrointestinal TractOlatomide OlaniranPas encore d'évaluation
- Abdominal AnatomyDocument39 pagesAbdominal AnatomyRahul MandhanPas encore d'évaluation
- Embryo Development Ofthe GI SytermDocument11 pagesEmbryo Development Ofthe GI SytermKingPas encore d'évaluation
- Small Intestine MMCDocument65 pagesSmall Intestine MMCWorku KiflePas encore d'évaluation
- Development of the Gastrointestinal TractDocument28 pagesDevelopment of the Gastrointestinal TractSaif100% (1)
- Small Intestine 2017Document78 pagesSmall Intestine 2017yasrul izadPas encore d'évaluation
- Digestive System EmbryologyDocument104 pagesDigestive System EmbryologyAlistair WalkerPas encore d'évaluation
- 1 Abdominal VisceraDocument45 pages1 Abdominal VisceraMero HamedPas encore d'évaluation
- Anatomy of PeritoneumDocument61 pagesAnatomy of PeritoneumFirdaus SeptiawanPas encore d'évaluation
- Development of the Gastrointestinal SystemDocument88 pagesDevelopment of the Gastrointestinal SystemBindiya MangarPas encore d'évaluation
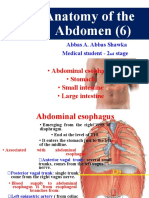
- Anatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineDocument34 pagesAnatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineBilal YimamPas encore d'évaluation
- The Small Intestine-1Document38 pagesThe Small Intestine-1ChiderahPas encore d'évaluation
- Development of Gastrointestinal SystemDocument29 pagesDevelopment of Gastrointestinal SystemrifkaraihanaPas encore d'évaluation
- Embryology Course VIII - Digestive SystemDocument47 pagesEmbryology Course VIII - Digestive SystemRawa MuhsinPas encore d'évaluation
- Digestive SystemDocument65 pagesDigestive SystemAdan ImanPas encore d'évaluation
- Surgical Anatomy of PeritoneumDocument63 pagesSurgical Anatomy of PeritoneumSuvarna RajPas encore d'évaluation
- Dr. Meidona - Development of Gastrointestinal System PDFDocument54 pagesDr. Meidona - Development of Gastrointestinal System PDFwkwkwkhhhhPas encore d'évaluation
- Ana SGD 15Document67 pagesAna SGD 15Bea ManzanoPas encore d'évaluation
- Gross Anatomy LiverDocument51 pagesGross Anatomy LiverDeny ShajiniPas encore d'évaluation
- G & D Lecture 9 Development of The Gi System Part 2 Spring 2018Document42 pagesG & D Lecture 9 Development of The Gi System Part 2 Spring 2018John H. SolomonPas encore d'évaluation
- Small IntestineDocument34 pagesSmall IntestineIAMSANWAR019170100% (1)
- Gastrointestinal AnatomyDocument70 pagesGastrointestinal AnatomyNatasya Ryani PurbaPas encore d'évaluation
- Development of The Gi SystemDocument6 pagesDevelopment of The Gi SystemKingPas encore d'évaluation
- ANAT 221 - PeritoneumDocument22 pagesANAT 221 - PeritoneumWisdom IkechukwuPas encore d'évaluation
- Lo 4Document7 pagesLo 4api-3803109Pas encore d'évaluation
- The PERITONEUMDocument27 pagesThe PERITONEUMEniola abdullahi AduagbaPas encore d'évaluation
- The Kidneys (Nephros) : FunctionsDocument6 pagesThe Kidneys (Nephros) : FunctionsOjambo FlaviaPas encore d'évaluation
- Anatomy of Liver and Pancreas by Kazim AliDocument32 pagesAnatomy of Liver and Pancreas by Kazim AliAhmad KhanPas encore d'évaluation
- PeritoneumDocument8 pagesPeritoneumDavid BadaruPas encore d'évaluation
- Peritoneum, Peritoneal Cavity, and Diaphragm 11-6-15-1Document67 pagesPeritoneum, Peritoneal Cavity, and Diaphragm 11-6-15-1Deny ShajiniPas encore d'évaluation
- PeritoneumDocument39 pagesPeritoneumtuhinsinghPas encore d'évaluation
- Anatomy of the PeritoneumDocument11 pagesAnatomy of the PeritoneumLeona Tinotenda ManjeruPas encore d'évaluation
- Structures of The ForegutDocument13 pagesStructures of The ForegutJatan KothariPas encore d'évaluation
- Abdomen - Esophagus To ColonDocument42 pagesAbdomen - Esophagus To ColonBibek GajmerPas encore d'évaluation
- GI Anatomy Golden!Document39 pagesGI Anatomy Golden!Ayodeji SotimehinPas encore d'évaluation
- Anatomi Dan Histologi Saluran Cerna BawahDocument20 pagesAnatomi Dan Histologi Saluran Cerna BawahIlhamDevirxaPas encore d'évaluation
- Anatomy Stomach & Duodenum: by Mekonnen.A (R1)Document46 pagesAnatomy Stomach & Duodenum: by Mekonnen.A (R1)Tsega WesenPas encore d'évaluation
- Physiology of Lower GI TractDocument180 pagesPhysiology of Lower GI TractIcarus WingsPas encore d'évaluation
- DuodenumDocument37 pagesDuodenumAayush BhattaPas encore d'évaluation
- Abdomen - FRCEM SuccessDocument275 pagesAbdomen - FRCEM SuccessAbin ThomasPas encore d'évaluation
- Peritoneum. Development of The Digestive System: Department of Human Anatomy Lecturer Dr. Globa LilianDocument24 pagesPeritoneum. Development of The Digestive System: Department of Human Anatomy Lecturer Dr. Globa LilianCristina GrajdeanPas encore d'évaluation
- Accessory GlandsDocument55 pagesAccessory GlandsMaxamed Faarax XaashiPas encore d'évaluation
- Peritoneum: General FeaturesDocument92 pagesPeritoneum: General FeaturestuhinsinghPas encore d'évaluation
- PANCREAS ANATOMY & PHYSIOLOGYDocument96 pagesPANCREAS ANATOMY & PHYSIOLOGYchandana pallavaPas encore d'évaluation
- Digestive SystemDocument6 pagesDigestive SystemDorence SimuntalaPas encore d'évaluation
- Large Intestine PIMSR-Dr - Gosai 2022Document40 pagesLarge Intestine PIMSR-Dr - Gosai 2022Dr.B.B.GosaiPas encore d'évaluation
- Development and rotation of the midgutDocument18 pagesDevelopment and rotation of the midgutMaster MastrikerPas encore d'évaluation
- Anatomy and Histology Gaster - DuodenumDocument149 pagesAnatomy and Histology Gaster - DuodenumRevila AuliaPas encore d'évaluation
- The StomachDocument3 pagesThe StomachSanjay KishorePas encore d'évaluation
- Gross Anatomy: Abdomen 4 Kidneys, Ureter and Urinary BladderDocument74 pagesGross Anatomy: Abdomen 4 Kidneys, Ureter and Urinary BladderBibek GajmerPas encore d'évaluation
- The pancreas: Anatomy, functions, and clinical relevanceDocument14 pagesThe pancreas: Anatomy, functions, and clinical relevanceTanveer AhmadPas encore d'évaluation
- Peritoneum & Peritoneal Cavity PresentationDocument59 pagesPeritoneum & Peritoneal Cavity Presentationsaint thuggerPas encore d'évaluation
- Digestive SystemDocument106 pagesDigestive SystemAuza Moses IbrahimPas encore d'évaluation
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Penyakit Kulit Akibat VirusDocument23 pagesPenyakit Kulit Akibat VirusLuna LitamiPas encore d'évaluation
- Chorn DDocument43 pagesChorn DLuna LitamiPas encore d'évaluation
- A 5 Year Record-Based Descriptive Study From A Tertiary Care Centre in South IndiaDocument6 pagesA 5 Year Record-Based Descriptive Study From A Tertiary Care Centre in South IndiaLuna LitamiPas encore d'évaluation
- 02.zainuri Anatomi Organ Reproduksi BaruDocument84 pages02.zainuri Anatomi Organ Reproduksi BaruDienda AleashaPas encore d'évaluation
- Kuliah Histologi MataDocument47 pagesKuliah Histologi MataLuna Litami100% (1)
- Jurnal FixDocument5 pagesJurnal FixLuna LitamiPas encore d'évaluation
- Assessing The Relationship Between Vector Indices andDocument11 pagesAssessing The Relationship Between Vector Indices andLuna LitamiPas encore d'évaluation
- Tumor Mata, Hidung, KulitDocument54 pagesTumor Mata, Hidung, KulitLuna LitamiPas encore d'évaluation
- DR Zainuri Kelainan Genetik 2013Document71 pagesDR Zainuri Kelainan Genetik 2013Luna LitamiPas encore d'évaluation
- Efficacy of Treatment For Somatoform DisordersDocument8 pagesEfficacy of Treatment For Somatoform DisordersRakhmad HarissonoPas encore d'évaluation
- KORNEA - DR Artati Des2012Document34 pagesKORNEA - DR Artati Des2012Luna LitamiPas encore d'évaluation
- KORNEA - DR Artati Des2012Document34 pagesKORNEA - DR Artati Des2012Luna LitamiPas encore d'évaluation
- PLEURA Efusion KuliahLDocument46 pagesPLEURA Efusion KuliahLLuna LitamiPas encore d'évaluation
- Kuliah Anatomi RespirasiDocument111 pagesKuliah Anatomi RespirasiLuna LitamiPas encore d'évaluation
- Dr Djoko Utomo SpM Guide Cataract FormationDocument27 pagesDr Djoko Utomo SpM Guide Cataract FormationLuna LitamiPas encore d'évaluation
- Research: Women 'S Views About Management and Cause of Urinary Tract Infection: Qualitative Interview StudyDocument7 pagesResearch: Women 'S Views About Management and Cause of Urinary Tract Infection: Qualitative Interview StudyLuna LitamiPas encore d'évaluation
- Action Potential 3Document38 pagesAction Potential 3Luna LitamiPas encore d'évaluation
- DR Zainuri - Embriologi Dan Topografi Trac RespiratoriusDocument62 pagesDR Zainuri - Embriologi Dan Topografi Trac RespiratoriusLuna LitamiPas encore d'évaluation
- ResearchDocument5 pagesResearchLuna LitamiPas encore d'évaluation
- Kuliah 3 Uii Copd, AsthmaDocument53 pagesKuliah 3 Uii Copd, AsthmaLuna LitamiPas encore d'évaluation
- Kuliah 3 Uii Copd, AsthmaDocument53 pagesKuliah 3 Uii Copd, AsthmaLuna LitamiPas encore d'évaluation
- PLEURA Efusion KuliahLDocument46 pagesPLEURA Efusion KuliahLLuna LitamiPas encore d'évaluation
- KULIAH 1 UTI UrinaryTractDisordersDocument55 pagesKULIAH 1 UTI UrinaryTractDisordersLuna LitamiPas encore d'évaluation
- Jurnal Rumah SakitDocument10 pagesJurnal Rumah SakitLuna LitamiPas encore d'évaluation
- Caregiving Body TemperatureDocument69 pagesCaregiving Body TemperatureDanny Line100% (1)
- ACRC 40k Surrogacy Program Fees Overview. (2305)Document4 pagesACRC 40k Surrogacy Program Fees Overview. (2305)jiawhu2008Pas encore d'évaluation
- Copy3-Obgyn Final Base LvivtechDocument3 466 pagesCopy3-Obgyn Final Base LvivtechHart ElettPas encore d'évaluation
- 464 2016 Article 5245Document54 pages464 2016 Article 5245Sintia KristianiPas encore d'évaluation
- Soap HamilDocument5 pagesSoap Hamilusnal.4iniPas encore d'évaluation
- RUP Baseline Questionnaire FINALDocument3 pagesRUP Baseline Questionnaire FINALNora MustacisaPas encore d'évaluation
- Dose Conversions of ErythromycinDocument4 pagesDose Conversions of ErythromycinastridridddddddsdPas encore d'évaluation
- Daudon CVDocument2 pagesDaudon CVmariusPas encore d'évaluation
- PROFILE of Virk HospitalDocument14 pagesPROFILE of Virk HospitalwittyvishwasPas encore d'évaluation
- Scoliosis SOS - Correcting CurvatureDocument3 pagesScoliosis SOS - Correcting CurvatureDaiyKramerPas encore d'évaluation
- MRKH MenopauseDocument3 pagesMRKH Menopausediudiu93Pas encore d'évaluation
- Pathophysiology of SyncopeDocument2 pagesPathophysiology of SyncopeErwin Chiquete, MD, PhDPas encore d'évaluation
- 7.dark Circles CausesDocument5 pages7.dark Circles CausesMohanraj VenuPas encore d'évaluation
- 28 Neurovasculature Conference For StudentsDocument36 pages28 Neurovasculature Conference For Students8jm6dhjdcpPas encore d'évaluation
- Community Health NursingDocument9 pagesCommunity Health NursingtheglobalnursingPas encore d'évaluation
- Masquerade SyndromesDocument10 pagesMasquerade Syndromestony_chrisPas encore d'évaluation
- International Conference On Applied Science and HealthDocument6 pagesInternational Conference On Applied Science and HealthDerison MarsinovaPas encore d'évaluation
- Surgical Specimen Management: A Descriptive Study of 648 Adverse Events and Near MissesDocument7 pagesSurgical Specimen Management: A Descriptive Study of 648 Adverse Events and Near MissesRubia Sari Mamanya HaristPas encore d'évaluation
- Multiple Birth FactsDocument6 pagesMultiple Birth FactsElliotPianoPas encore d'évaluation
- Should the UK allow commercial surrogacy to curb health risks to Indian surrogatesDocument8 pagesShould the UK allow commercial surrogacy to curb health risks to Indian surrogatestanmaya_purohitPas encore d'évaluation
- MSU Nursing Roles MatrixDocument2 pagesMSU Nursing Roles MatrixSitty Aizah MangotaraPas encore d'évaluation
- Transcutaneous Electrical Nerve Stimulation (Tens) and Pain ManagementDocument54 pagesTranscutaneous Electrical Nerve Stimulation (Tens) and Pain ManagementhashfiluthfihPas encore d'évaluation
- Wound DehiscenceDocument3 pagesWound DehiscenceDanickz Natura MallariPas encore d'évaluation
- Index of :public:Books:BioMedDocument167 pagesIndex of :public:Books:BioMedCharlie33% (3)
- Labor Curve & Partograph GuideDocument50 pagesLabor Curve & Partograph GuideJhervy VillanuevaPas encore d'évaluation
- Waht-Cri-005 V2Document17 pagesWaht-Cri-005 V2Innas DoankPas encore d'évaluation
- Head To Toe Assessment NRS 111Document4 pagesHead To Toe Assessment NRS 111Danielle Shull100% (2)
- 5663 PDFDocument7 pages5663 PDFwaelPas encore d'évaluation
- Bhore Committee 1946Document32 pagesBhore Committee 1946saritatelma100% (1)
- Anthony Filly CVDocument5 pagesAnthony Filly CVapi-289727140Pas encore d'évaluation