Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Alexanders Care Patient Surgery 16th Rothrock Test BankDocument10 pagesAlexanders Care Patient Surgery 16th Rothrock Test BankfahedqPas encore d'évaluation
- The BreastDocument72 pagesThe BreastMohammad_Islam87Pas encore d'évaluation
- Physiopathology SyllabusDocument1 pagePhysiopathology SyllabusMohammad_Islam87Pas encore d'évaluation
- Lecture 17 DiabetesDocument51 pagesLecture 17 DiabetesMohammad_Islam87Pas encore d'évaluation
- Lecture 18 Upper Digestive DiseasesDocument63 pagesLecture 18 Upper Digestive DiseasesMohammad_Islam87Pas encore d'évaluation
- The LymphomasDocument46 pagesThe LymphomasMohammad_Islam87Pas encore d'évaluation
- Lecture 20 CarcinogenesisDocument84 pagesLecture 20 CarcinogenesisMohammad_Islam87100% (1)
- Pharmacology Lecture 12-5-2009, OpiodsDocument18 pagesPharmacology Lecture 12-5-2009, OpiodsMohammad_Islam87Pas encore d'évaluation
- Curst Um Abd EnglDocument10 pagesCurst Um Abd EnglMohammad_Islam87Pas encore d'évaluation
- Abdominal HerniaeDocument66 pagesAbdominal HerniaeMohammad_Islam87Pas encore d'évaluation
- Plastic SurgeryDocument11 pagesPlastic SurgeryMohammad_Islam87Pas encore d'évaluation
- Liver Curs 2009Document215 pagesLiver Curs 2009Mohammad_Islam87Pas encore d'évaluation
- ?#ry%oefr: - J4 @,8/ MryDocument15 pages?#ry%oefr: - J4 @,8/ MryMohammad_Islam87Pas encore d'évaluation
- AnaemiaDocument83 pagesAnaemiaMohammad_Islam87100% (2)
- Pharmacology Lecture 19-5-2009, NSAIDSDocument19 pagesPharmacology Lecture 19-5-2009, NSAIDSMohammad_Islam87Pas encore d'évaluation
- Borcane TumorDocument14 pagesBorcane TumorMohammad_Islam87Pas encore d'évaluation
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadDocument25 pagesMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87Pas encore d'évaluation
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractDocument29 pagesMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87Pas encore d'évaluation
- Morphopathology Macroscopy (Romanian-Batch)Document187 pagesMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadDocument19 pagesMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87Pas encore d'évaluation
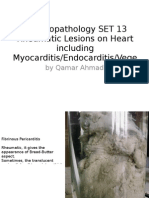
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeDocument25 pagesMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87Pas encore d'évaluation
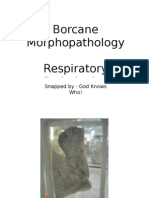
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocument11 pagesBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Pas encore d'évaluation
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocument7 pagesBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- Pharmacology Lecture Diuretic Agents (High Quality)Document15 pagesPharmacology Lecture Diuretic Agents (High Quality)Mohammad_Islam87Pas encore d'évaluation
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadDocument18 pagesMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87Pas encore d'évaluation
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocument7 pagesBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Pas encore d'évaluation
- Workshop 20Document2 pagesWorkshop 20Mohammad_Islam87Pas encore d'évaluation
- Pharmacology Lecture 5-5-2009Document15 pagesPharmacology Lecture 5-5-2009Mohammad_Islam87Pas encore d'évaluation
- Conditions Presenting With Abdominal PainDocument69 pagesConditions Presenting With Abdominal PainaimanPas encore d'évaluation
- Workshop 19Document3 pagesWorkshop 19Mohammad_Islam87Pas encore d'évaluation
- Engl BUN - EditDocument167 pagesEngl BUN - EditMohammad_Islam87Pas encore d'évaluation
- ExodontiaDocument32 pagesExodontiaahmed amerPas encore d'évaluation
- AdrenalineDocument13 pagesAdrenalineMobahil AhmadPas encore d'évaluation
- Pschology 2Document35 pagesPschology 2Sarah Mae SaringanPas encore d'évaluation
- Nursing Health Assessment Guide: San Pedro CollegeDocument3 pagesNursing Health Assessment Guide: San Pedro CollegeRue Cheng MaPas encore d'évaluation
- Common Types of StrabismusDocument9 pagesCommon Types of Strabismustasya noerchaerunisaPas encore d'évaluation
- Steroid AbuseDocument7 pagesSteroid Abuseapi-400575655Pas encore d'évaluation
- Scabies NotesDocument9 pagesScabies NotesAvi ePas encore d'évaluation
- Coroflex® ISAR Neo1Document8 pagesCoroflex® ISAR Neo1Waseem KhalidPas encore d'évaluation
- RRLDocument4 pagesRRLKing-king Caballero50% (2)
- Hematologic EffectsDocument8 pagesHematologic EffectsGiralph NikkoPas encore d'évaluation
- JPediatrCritCare2167-4903094 133710Document18 pagesJPediatrCritCare2167-4903094 133710brajendra singhPas encore d'évaluation
- Antifungal and Antibacterial Activity of ExtractsDocument30 pagesAntifungal and Antibacterial Activity of ExtractsFrengkyPas encore d'évaluation
- Monday, October 06, 2014 EditionDocument12 pagesMonday, October 06, 2014 EditionFrontPageAfricaPas encore d'évaluation
- Medical Science Liaisons:: A Key To Driving Patient Access To New TherapiesDocument20 pagesMedical Science Liaisons:: A Key To Driving Patient Access To New TherapiesMunib Ur RehmanPas encore d'évaluation
- Concept and Application of Gene Mapping in Animal BreedingDocument9 pagesConcept and Application of Gene Mapping in Animal BreedingLucio MotaPas encore d'évaluation
- Quality of Life in Burn Injury PatientsDocument8 pagesQuality of Life in Burn Injury PatientsFaisal A. RaniPas encore d'évaluation
- Autonomic NeuropathyDocument20 pagesAutonomic NeuropathyRegina CaeciliaPas encore d'évaluation
- Balance, Posture and Body AlignmentDocument6 pagesBalance, Posture and Body AlignmenthahahahaaaaaaaPas encore d'évaluation
- Assessing Disease Severity and Quality of Life in Psoriasis Patients: A Comprehensive StudyDocument16 pagesAssessing Disease Severity and Quality of Life in Psoriasis Patients: A Comprehensive StudyIJAR JOURNALPas encore d'évaluation
- Anatomy of The Ear TMN NewDocument26 pagesAnatomy of The Ear TMN NewMerriPas encore d'évaluation
- Covid-19: Asian Xenophobia and RacismDocument12 pagesCovid-19: Asian Xenophobia and RacismNayab Binte Fiaz100% (1)
- Garcia, Nehemiah B. BSN 2Y2-2A: Ncma 219 Rle Course Task # 2Document3 pagesGarcia, Nehemiah B. BSN 2Y2-2A: Ncma 219 Rle Course Task # 2Mushy_ayaPas encore d'évaluation
- STS Video ScriptDocument2 pagesSTS Video ScriptCynthia Y De VeraPas encore d'évaluation
- December 2018 Ophthalmic PearlsDocument2 pagesDecember 2018 Ophthalmic PearlsFathirPas encore d'évaluation
- Intro To AromatherapyDocument58 pagesIntro To AromatherapyrameshgounderPas encore d'évaluation
- Germ Theory of Diseases Von PlencizDocument2 pagesGerm Theory of Diseases Von PlencizAamni SinghPas encore d'évaluation
- 6: Diagnostic Microbiology and Laboratory Methods - Pocket DentistryDocument9 pages6: Diagnostic Microbiology and Laboratory Methods - Pocket Dentistrykam LinPas encore d'évaluation
- Homemade MethcathinoneDocument16 pagesHomemade MethcathinoneDaria Schka100% (1)
- Balleine and Doherty 2010 - NeuropsychopharmacologyDocument22 pagesBalleine and Doherty 2010 - NeuropsychopharmacologySirathpulPas encore d'évaluation