Vous aimerez peut-être aussi
- Systemic FluorideDocument7 pagesSystemic FluoridemaryamfaidelPas encore d'évaluation
- Flourides and FluoridationDocument38 pagesFlourides and FluoridationmisdduaaPas encore d'évaluation
- FluoridesDocument54 pagesFluoridesNAUMAN SHAHPas encore d'évaluation
- Lec 9 PDFDocument7 pagesLec 9 PDFFlorida ManPas encore d'évaluation
- FluoridesDocument52 pagesFluoridesRahel CharikarPas encore d'évaluation
- Dr. Ali Fahad Al-Fatlawi Community Dentistry LEC: 6Document3 pagesDr. Ali Fahad Al-Fatlawi Community Dentistry LEC: 6مؤمل رياض سعد كاظمPas encore d'évaluation
- DR Mona Mustafa Bds - MD - DrmeDocument58 pagesDR Mona Mustafa Bds - MD - Drmeعبدالمحسن العيسىPas encore d'évaluation
- Flouride Map PDFDocument1 pageFlouride Map PDFTesfa AkliluPas encore d'évaluation
- Flouride in Dentistry by Ammar MohammedDocument10 pagesFlouride in Dentistry by Ammar Mohammedعمار محمد عباسPas encore d'évaluation
- Fluoridation Prevention MethodsDocument6 pagesFluoridation Prevention MethodsFlorida ManPas encore d'évaluation
- 3 FluorideDocument26 pages3 Fluoridemrbyy619Pas encore d'évaluation
- Topical and Systemic FluorideDocument12 pagesTopical and Systemic Fluoridemidoo47Pas encore d'évaluation
- FluoriosisDocument73 pagesFluoriosisnathanielge19Pas encore d'évaluation
- National Programme For Prevention and Control of FluorosisDocument49 pagesNational Programme For Prevention and Control of FluorosisveereshPas encore d'évaluation
- AppendicesDocument8 pagesAppendicesريام الموسويPas encore d'évaluation
- Fluoride in Dentistry: DR Mona Mustafa Bds - MDDocument61 pagesFluoride in Dentistry: DR Mona Mustafa Bds - MDTasneem DakkakPas encore d'évaluation
- Role of Fluorides in Preventing Tooth DecayDocument54 pagesRole of Fluorides in Preventing Tooth DecayShanaz ShaxawanPas encore d'évaluation
- Fluoride TherapyDocument4 pagesFluoride TherapyمعتزباللهPas encore d'évaluation
- 1.1 BackgroundDocument43 pages1.1 Backgroundகாளையின் காதலன்Pas encore d'évaluation
- TOXICITY of FLOURIDESDocument45 pagesTOXICITY of FLOURIDESNavneet KaurPas encore d'évaluation
- (Fluoride in Dentistry) : Prevention and Controlling of Dental CariesDocument32 pages(Fluoride in Dentistry) : Prevention and Controlling of Dental Cariesفواز نميرPas encore d'évaluation
- Fluoride Therapy: Latest RevisionDocument4 pagesFluoride Therapy: Latest RevisionHamdy AlmaghrabyPas encore d'évaluation
- Fluoride ReviewDocument5 pagesFluoride ReviewAbelia ABPas encore d'évaluation
- Guideline On Fluoride Therapy: Review Council Latest RevisionDocument4 pagesGuideline On Fluoride Therapy: Review Council Latest RevisionThesya Aulia GeovanyPas encore d'évaluation
- G Fluoridetherapy PDFDocument4 pagesG Fluoridetherapy PDFChandrika VeerareddyPas encore d'évaluation
- Guide to Fluoride TherapyDocument4 pagesGuide to Fluoride TherapymirfanulhaqPas encore d'évaluation
- Fluoride's Role in Oral HealthDocument11 pagesFluoride's Role in Oral HealthnoorPas encore d'évaluation
- Fluorides: Studentica: Dora Maršanić Kolegij: Engleski Jezik Voditelj Kolegija: Doc. Dr. Sc. Arijana Krišković, ProfDocument27 pagesFluorides: Studentica: Dora Maršanić Kolegij: Engleski Jezik Voditelj Kolegija: Doc. Dr. Sc. Arijana Krišković, ProfBokiPas encore d'évaluation
- Who Ced PheDocument8 pagesWho Ced PheMuhammad RizwanPas encore d'évaluation
- Systemic Fluorides Lesson PlanDocument34 pagesSystemic Fluorides Lesson PlanAneesa AzeezPas encore d'évaluation
- BP FluorideTherapyDocument4 pagesBP FluorideTherapyKavana SrinivasPas encore d'évaluation
- Fluorides in Dentistry: Dental Caries Prevention and ControlDocument5 pagesFluorides in Dentistry: Dental Caries Prevention and ControlFlorida ManPas encore d'évaluation
- Fluoride Treatment GuideDocument47 pagesFluoride Treatment GuideNathnael GebeyehuPas encore d'évaluation
- Preventive DentistryDocument7 pagesPreventive DentistryAyad IbrahimPas encore d'évaluation
- FluorideDocument50 pagesFluoriderajshreePas encore d'évaluation
- Water Fluoridation: Fluoridation Methods Used in Dental Caries PreventionDocument2 pagesWater Fluoridation: Fluoridation Methods Used in Dental Caries PreventionEdralene AntoyPas encore d'évaluation
- Fluorideindentistry 210630220303Document30 pagesFluorideindentistry 210630220303Fahad AliPas encore d'évaluation
- Prevention of Dental CariesDocument37 pagesPrevention of Dental CariesReda IsmaeelPas encore d'évaluation
- Fluoride Therapy: Latest RevisionDocument4 pagesFluoride Therapy: Latest RevisionLaura ZahariaPas encore d'évaluation
- Fluoride: Nature's Cavity FighterDocument11 pagesFluoride: Nature's Cavity FighterAya OsamaPas encore d'évaluation
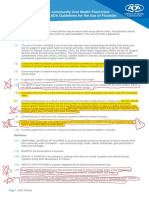
- Community Oral Health Promotion: Fluoride Use PolicyDocument5 pagesCommunity Oral Health Promotion: Fluoride Use PolicyTalat SultanaPas encore d'évaluation
- Fluoride in DentistryDocument42 pagesFluoride in DentistryAbhishek SoniPas encore d'évaluation
- Topikal Aplikasi FluorDocument7 pagesTopikal Aplikasi FluorYessy Natalia NataliaPas encore d'évaluation
- Nut FluorideDocument12 pagesNut FluorideBrandan SahnkovichPas encore d'évaluation
- Fluoride SourcesDocument1 pageFluoride SourcesFoysal SirazeePas encore d'évaluation
- PEDO Journal Review of Fluoride in Caries PreventionDocument8 pagesPEDO Journal Review of Fluoride in Caries PreventioncsryderPas encore d'évaluation
- Presentation On Mitigation of FluorosisDocument67 pagesPresentation On Mitigation of FluorosisViswa NathanPas encore d'évaluation
- De-fluoridation of Ground Water Using Impregnated AluminumDocument1 pageDe-fluoridation of Ground Water Using Impregnated AluminumAwais Ahmed JamaliPas encore d'évaluation
- Fluoride's role in preventing dental cariesDocument7 pagesFluoride's role in preventing dental cariesHaider F YehyaPas encore d'évaluation
- Epidemiology of Endemic Fluorosis: Causes, Effects and PreventionDocument15 pagesEpidemiology of Endemic Fluorosis: Causes, Effects and PreventionAli HaDi MohamedPas encore d'évaluation
- Dental FluorosisDocument5 pagesDental FluorosisAbdullah EhsanPas encore d'évaluation
- Terapia de Fluor AAPDDocument4 pagesTerapia de Fluor AAPDAndy HerreraPas encore d'évaluation
- Fluoride Lec 3 PDFDocument5 pagesFluoride Lec 3 PDFRick SanchezPas encore d'évaluation
- Dental FluorosisDocument70 pagesDental Fluorosiskaran89Pas encore d'évaluation
- AAPD Policy on Use of FluorideDocument2 pagesAAPD Policy on Use of FluorideAlexandraPortugalInfantasPas encore d'évaluation
- Anticaries AgentsDocument12 pagesAnticaries AgentsHridoyul IslamPas encore d'évaluation
- Fluoride: Drinking Ourselves to Death?: The Scientific Argument Against Water FluoridationD'EverandFluoride: Drinking Ourselves to Death?: The Scientific Argument Against Water FluoridationPas encore d'évaluation
- Epidemiologi Dental (Identifikasi Jurnal)Document6 pagesEpidemiologi Dental (Identifikasi Jurnal)Vina NuranisyahPas encore d'évaluation
- A Review of Contemporary DentifricesDocument11 pagesA Review of Contemporary DentifricesgabyPas encore d'évaluation
- Item DescriptionDocument736 pagesItem DescriptionSatyam Kumar100% (1)
- Comparative Evaluation of Antibacterial Efficacy.9Document6 pagesComparative Evaluation of Antibacterial Efficacy.9Shivani DubeyPas encore d'évaluation
- Everything You Need to Know About ToothpasteDocument20 pagesEverything You Need to Know About ToothpasteBrijesh KumarPas encore d'évaluation
- Mehak Chauhan Final ProjectDocument82 pagesMehak Chauhan Final ProjectvanshikaPas encore d'évaluation
- LUSSI, 2019. The Use of Fluoride For The Prevention of Dental Erosion and Erosive Tooth Wear in Children and Adolescents PDFDocument11 pagesLUSSI, 2019. The Use of Fluoride For The Prevention of Dental Erosion and Erosive Tooth Wear in Children and Adolescents PDFJohnatan MeirelesPas encore d'évaluation
- MKT 201 ProjectDocument29 pagesMKT 201 ProjectJareen RashaPas encore d'évaluation
- Comparitive Study Colgate and PepsodentDocument10 pagesComparitive Study Colgate and PepsodentSunil MathewsPas encore d'évaluation
- CloseupDocument4 pagesCloseupWilliam DsouzaPas encore d'évaluation
- Patanjali Products List With PriceDocument12 pagesPatanjali Products List With Priceshahib virenderPas encore d'évaluation
- Dental Caries A DiseaseDocument57 pagesDental Caries A Diseaseasti finda100% (1)
- Cassanova's Annual Sale and Savings EventDocument7 pagesCassanova's Annual Sale and Savings Eventahmad abu bakarPas encore d'évaluation
- Science Subject For Senior High:: ChemistryDocument55 pagesScience Subject For Senior High:: ChemistryFan of YouPas encore d'évaluation
- Efektivitas Pasta Gigi Herbal vs Non Herbal Mengurangi PlakDocument6 pagesEfektivitas Pasta Gigi Herbal vs Non Herbal Mengurangi PlakEndah SuryaniPas encore d'évaluation
- Preventive Dentistry: Other Caries Preventive FactorsDocument70 pagesPreventive Dentistry: Other Caries Preventive FactorsKK AgarwallPas encore d'évaluation
- Dental Pharmacology: Drugs for Oral Hygiene, Root Canal Therapy, and Periodontal DiseasesDocument44 pagesDental Pharmacology: Drugs for Oral Hygiene, Root Canal Therapy, and Periodontal DiseasesMalatesh Sudharshan100% (1)
- Project Report On Apollo Earthmovers LimitedDocument40 pagesProject Report On Apollo Earthmovers LimitedRaHul RathodPas encore d'évaluation
- WinS Monitoring System - Blank v2017-06-04Document16 pagesWinS Monitoring System - Blank v2017-06-04Marie Fe EgarPas encore d'évaluation
- QCU WWAOS Enterprise Marketing and Production PlanDocument144 pagesQCU WWAOS Enterprise Marketing and Production PlanJohn Andrie EscobidoPas encore d'évaluation
- Colgate Marketing ReportDocument16 pagesColgate Marketing ReportRaja GuruPas encore d'évaluation
- 6 Ihc Halal ChampionDocument39 pages6 Ihc Halal ChampionCheAzahariCheAhmadPas encore d'évaluation
- GFTR 9Document52 pagesGFTR 9vishal vishalPas encore d'évaluation
- Nathalie Gem E. Juanillo: Giving BackDocument2 pagesNathalie Gem E. Juanillo: Giving BackMaria SarsabaPas encore d'évaluation
- Baking Soda As An Abrasive in Toothpastes: Mechanism of Action and Safety and Effectiveness ConsiderationsDocument7 pagesBaking Soda As An Abrasive in Toothpastes: Mechanism of Action and Safety and Effectiveness ConsiderationsGhina Mukti LuthfiaPas encore d'évaluation
- PC Kao 2007Document29 pagesPC Kao 2007amw3100% (2)
- CB Assignment Dolfi Singla 17ADocument3 pagesCB Assignment Dolfi Singla 17AsandeeptiiftPas encore d'évaluation
- Assignment On Strategic Marketing ManagementDocument14 pagesAssignment On Strategic Marketing ManagementUmer waleedPas encore d'évaluation
- Fragments: On Dentistry. Ander MonsonDocument23 pagesFragments: On Dentistry. Ander MonsonUrsula Fuentesberain100% (1)
- Dental Kin Gingival Complex Gums Toothpaste 75mlDocument1 pageDental Kin Gingival Complex Gums Toothpaste 75mlDavid BurkePas encore d'évaluation