Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
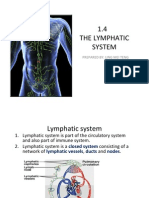
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDocument15 pages1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingPas encore d'évaluation
- Radiation Biology: Presented By: Aarya.H.NairDocument83 pagesRadiation Biology: Presented By: Aarya.H.NairAARYAPas encore d'évaluation
- ICSE Class 10 Biology Previous Year Question Paper 2011 PDFDocument9 pagesICSE Class 10 Biology Previous Year Question Paper 2011 PDFmohammedPas encore d'évaluation
- Metabolism of DisaccharidesDocument15 pagesMetabolism of DisaccharidesminaPas encore d'évaluation
- Assessing Lateral Hip StabilityDocument7 pagesAssessing Lateral Hip StabilityCristian Alejandro Flores PinuerPas encore d'évaluation
- Introduction to MedicineDocument156 pagesIntroduction to MedicineEshetu BizunehPas encore d'évaluation
- Test Bank For Essentials of Psychiatric Mental Health Nursing 7th Edition Mary C TownsendDocument15 pagesTest Bank For Essentials of Psychiatric Mental Health Nursing 7th Edition Mary C TownsendVanessa Martin100% (30)
- Glycolysis and cellular respiration overviewDocument3 pagesGlycolysis and cellular respiration overviewPaul PanizaPas encore d'évaluation
- Biochemistry QuizDocument28 pagesBiochemistry Quizsanjviews100% (3)
- The Third International Consensus Definitions For Sepsis and Septic Shock Sepsis-3 - JAMA 2016Document10 pagesThe Third International Consensus Definitions For Sepsis and Septic Shock Sepsis-3 - JAMA 2016Miguel Angel Quiroz CristobalPas encore d'évaluation
- 2018 Biology Exercises For SPM (Chapter6 & Chapter7)Document15 pages2018 Biology Exercises For SPM (Chapter6 & Chapter7)Kuen Jian LinPas encore d'évaluation
- Anatomy of The Rat The Nervous SystemDocument61 pagesAnatomy of The Rat The Nervous SystemBelleopsisPas encore d'évaluation
- Supranuclear Control Opf Eye MovementsDocument162 pagesSupranuclear Control Opf Eye Movementsknowledgeguruos179Pas encore d'évaluation
- The Developing Child - The First Seven Years - EbookDocument141 pagesThe Developing Child - The First Seven Years - Ebookall-natural-nutPas encore d'évaluation
- Lecture 8 - 30.12.2022Document17 pagesLecture 8 - 30.12.2022Adnan Mohammad Adnan HailatPas encore d'évaluation
- How Sleeping Positions Impact Sleep Quality and HealthDocument2 pagesHow Sleeping Positions Impact Sleep Quality and HealthNeelesh Suteri0% (1)
- Tetralogy of Fallot Everything You Wanted To Know But Were Afraid To AskDocument8 pagesTetralogy of Fallot Everything You Wanted To Know But Were Afraid To AsksofiaPas encore d'évaluation
- Circulatory System: Heart, Blood Vessels & Their FunctionsDocument17 pagesCirculatory System: Heart, Blood Vessels & Their FunctionskangaanushkaPas encore d'évaluation
- Paragraph Development ExerciseDocument6 pagesParagraph Development ExerciseSYAFINAS SALAM100% (1)
- Worksheet - Dna Protein SynthesisDocument2 pagesWorksheet - Dna Protein Synthesisapi-270403367100% (1)
- Comparative Study The Effect of Induction of General Anesthesia With Propofol Versus Thiopentone in Pediatric Age Group On Cardiovascular SystemDocument8 pagesComparative Study The Effect of Induction of General Anesthesia With Propofol Versus Thiopentone in Pediatric Age Group On Cardiovascular SystemCentral Asian StudiesPas encore d'évaluation
- BioSignature Review - Are Hormones The Key To Weight LossDocument19 pagesBioSignature Review - Are Hormones The Key To Weight LossVladimir OlefirenkoPas encore d'évaluation
- Anatomy 2ND de BachilleratoDocument24 pagesAnatomy 2ND de BachilleratoAlexander IntriagoPas encore d'évaluation
- Aids 2013Document404 pagesAids 2013kovaron80Pas encore d'évaluation
- GIT Physio D&R AgamDocument67 pagesGIT Physio D&R Agamvisweswar030406Pas encore d'évaluation
- NCP of CavDocument3 pagesNCP of CavHenry Roque TagalagPas encore d'évaluation
- Nicotrol InhalerDocument19 pagesNicotrol InhalerdebysiskaPas encore d'évaluation
- 1-Aarogyam 1.2 - PO4080828012-204Document10 pages1-Aarogyam 1.2 - PO4080828012-204jannyyatinPas encore d'évaluation
- Pe Lecture NotesDocument7 pagesPe Lecture NotesAnonymous LJrX4dzPas encore d'évaluation