Vous aimerez peut-être aussi
- Course: Medical Surgical Nursing Ii Course Code: NSC 322 Topic: Leukamia Lecturer: Mrs Chukwu Date: Tuesday, 7Th June, 2022Document13 pagesCourse: Medical Surgical Nursing Ii Course Code: NSC 322 Topic: Leukamia Lecturer: Mrs Chukwu Date: Tuesday, 7Th June, 2022Leo D' GreatPas encore d'évaluation
- Leukemia PDFDocument63 pagesLeukemia PDFErfan Syahid AzhariPas encore d'évaluation
- Aspergillus SP As Aflatoxin Producers in Grains and FeedsDocument30 pagesAspergillus SP As Aflatoxin Producers in Grains and FeedsNur QistinaPas encore d'évaluation
- Clinical Presentation, Pathologic Features, Diagnosis, and Differential Diagnosis of Chronic Lymphocytic Leukemia - UpToDateDocument23 pagesClinical Presentation, Pathologic Features, Diagnosis, and Differential Diagnosis of Chronic Lymphocytic Leukemia - UpToDateJosé Martínez100% (1)
- Genetic Basis of Disease PMDocument79 pagesGenetic Basis of Disease PMsunday daniel100% (1)
- Acute Lymphoblastic Leukemia (ALL)Document14 pagesAcute Lymphoblastic Leukemia (ALL)Med PhuongPas encore d'évaluation
- Gluten Sensitivity, Coeliac Disease and Brain HealthDocument87 pagesGluten Sensitivity, Coeliac Disease and Brain HealthAmy Ruskoski HendersonPas encore d'évaluation
- Hematopoietic System PathologyDocument78 pagesHematopoietic System PathologyNuhu SibaPas encore d'évaluation
- Blood DisordersDocument21 pagesBlood Disordersapi-448398971Pas encore d'évaluation
- Lymphoid NeoplasmsDocument52 pagesLymphoid NeoplasmsAmalia Riska GPas encore d'évaluation
- Lymphomas and LeukemiasDocument27 pagesLymphomas and LeukemiasgracePas encore d'évaluation
- Chemotherapy For Gynecologic CancerDocument69 pagesChemotherapy For Gynecologic CancerBEREKET100% (1)
- Case Study For LeukemiaDocument5 pagesCase Study For LeukemiaGabbii CincoPas encore d'évaluation
- Bone Marrow TransplantDocument8 pagesBone Marrow TransplantPSRI hospitalPas encore d'évaluation
- Chapter 13 Neoplastic Proliferations of White CellsDocument16 pagesChapter 13 Neoplastic Proliferations of White CellsOmar100% (1)
- Rare Kidney Cancer in ChildrenDocument12 pagesRare Kidney Cancer in ChildrenKath CamachoPas encore d'évaluation
- Oncology NotesDocument7 pagesOncology NotesRochel Mae LomedaPas encore d'évaluation
- Anorectal Suppuration 9.7.11!1!1Document50 pagesAnorectal Suppuration 9.7.11!1!1Shantu Shirurmath100% (2)
- Mastectomy patient chemotherapy side effects NCLEX reviewDocument4 pagesMastectomy patient chemotherapy side effects NCLEX reviewTinPas encore d'évaluation
- WBC Pathology: Lecturer: Associate Professor T. A. GrekovaDocument49 pagesWBC Pathology: Lecturer: Associate Professor T. A. GrekovaFaheem MusthafaPas encore d'évaluation
- WBC DisorderDocument24 pagesWBC DisorderNirav SharmaPas encore d'évaluation
- Acute Lymphoblastic Leukemia QuestionsDocument22 pagesAcute Lymphoblastic Leukemia Questionsđoàn lươngPas encore d'évaluation
- Hemophilia ADocument8 pagesHemophilia AroxhencaPas encore d'évaluation
- Blood Clotting Mechanisms and Thrombolytic TherapyDocument3 pagesBlood Clotting Mechanisms and Thrombolytic TherapyLindsey SimmonsPas encore d'évaluation
- Life Cycle and Prevention of Ascaris Lumbricoides InfectionDocument6 pagesLife Cycle and Prevention of Ascaris Lumbricoides InfectionPika PearlasPas encore d'évaluation
- Leukemia: Dr. Isbandiyah SPPD Bag. Ilmu Penyakit Dalam Umm MalangDocument26 pagesLeukemia: Dr. Isbandiyah SPPD Bag. Ilmu Penyakit Dalam Umm MalangSemesta0% (1)
- Complication of Blood TransfusionDocument5 pagesComplication of Blood TransfusionChey Ochy ApriliaPas encore d'évaluation
- Acute Leukemia Types and TreatmentDocument22 pagesAcute Leukemia Types and TreatmentFelix Allen100% (1)
- Hematologic SystemDocument81 pagesHematologic Systemseigelystic100% (23)
- What Is A Bone Marrow Transplant?Document4 pagesWhat Is A Bone Marrow Transplant?Krisna AgustiniPas encore d'évaluation
- All PPT FinalDocument58 pagesAll PPT FinalRobert RealonPas encore d'évaluation
- Stem Cell TransplantationDocument13 pagesStem Cell TransplantationMylls MondejarPas encore d'évaluation
- Reactive ArthritisDocument3 pagesReactive ArthritisMohammadAbuelhaijaPas encore d'évaluation
- Blood Transfusion PDFDocument20 pagesBlood Transfusion PDFalaamorsyPas encore d'évaluation
- Acute Lymphoblastic LeukemiaDocument25 pagesAcute Lymphoblastic Leukemiaapi-396564080Pas encore d'évaluation
- Cancer OverviewDocument10 pagesCancer Overviewampogison08Pas encore d'évaluation
- Immune System Docs 2019Document13 pagesImmune System Docs 2019David DavidPas encore d'évaluation
- Causes and Types of Rapidly Progressive GlomerulonephritisDocument28 pagesCauses and Types of Rapidly Progressive GlomerulonephritisPaul SinsPas encore d'évaluation
- Practice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearDocument44 pagesPractice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearSundarPas encore d'évaluation
- Cervical CancerDocument2 pagesCervical CancerLicio LentimoPas encore d'évaluation
- Rheumatoid ArthritisDocument29 pagesRheumatoid ArthritisTamim IshtiaquePas encore d'évaluation
- Derma Report Contact DermatitisDocument25 pagesDerma Report Contact DermatitisYusnida RahmawatiPas encore d'évaluation
- Embryo Lab Exercise 1Document7 pagesEmbryo Lab Exercise 1Karmina Santos100% (1)
- Parapneumonic Pleural Effusions and Empyema Thoracis: Causes, Symptoms and TreatmentDocument4 pagesParapneumonic Pleural Effusions and Empyema Thoracis: Causes, Symptoms and TreatmentLorentina Den PanjaitanPas encore d'évaluation
- Spleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementDocument53 pagesSpleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementMuhammad SaadPas encore d'évaluation
- Antineoplastic Agents 2011 Dental MARCH-1Document41 pagesAntineoplastic Agents 2011 Dental MARCH-1BinayakSwainPas encore d'évaluation
- Leukaemia and Lymphoma Whats The DifferenceDocument7 pagesLeukaemia and Lymphoma Whats The Differencepaul_calburean7899Pas encore d'évaluation
- Fluid & Electrolyte BalancesDocument44 pagesFluid & Electrolyte BalancesTri RachmadijantoPas encore d'évaluation
- 2014 - Lecture - Pathology of The Small and Large IntestineDocument12 pages2014 - Lecture - Pathology of The Small and Large IntestinesammysandsongPas encore d'évaluation
- Joint Pain - ApproachDocument32 pagesJoint Pain - ApproachHassan Bin AjmalPas encore d'évaluation
- Idiopathic Thrombocytopenic Purpura (ITP)Document7 pagesIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiPas encore d'évaluation
- Haemophilia: DR Y S Vishnu Vardhan, PGDocument64 pagesHaemophilia: DR Y S Vishnu Vardhan, PGVishnu VardhanPas encore d'évaluation
- Polycythemia vera and secondary causes explainedDocument9 pagesPolycythemia vera and secondary causes explainedJoeven HilarioPas encore d'évaluation
- Essentials of Diagnosis and Treatment of Acute LeukemiaDocument16 pagesEssentials of Diagnosis and Treatment of Acute Leukemianouval_iqbalPas encore d'évaluation
- Anticancer Drugs: Pharmacology of Chemotherapy AgentsDocument126 pagesAnticancer Drugs: Pharmacology of Chemotherapy AgentsZaina MasriPas encore d'évaluation
- Upper GIT BleedingDocument69 pagesUpper GIT BleedingSoleh Ramly100% (1)
- Etiology of Cervical Cancer PDFDocument2 pagesEtiology of Cervical Cancer PDFBudPas encore d'évaluation
- Problem-based Approach to Gastroenterology and HepatologyD'EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisPas encore d'évaluation
- Disorders of Respiratory Function - Infections and Neoplasms - 2020Document17 pagesDisorders of Respiratory Function - Infections and Neoplasms - 2020Cres Padua QuinzonPas encore d'évaluation
- Disorders of Renal Function Calculi - UTIDocument21 pagesDisorders of Renal Function Calculi - UTICres Padua QuinzonPas encore d'évaluation
- Disorders of GIT - 2020-2021Document81 pagesDisorders of GIT - 2020-2021Cres Padua QuinzonPas encore d'évaluation
- Disorders of Arterial Circulation - 8Document42 pagesDisorders of Arterial Circulation - 8Cres Padua QuinzonPas encore d'évaluation
- Endocrine Disorders: Patho Phys Iolog yDocument20 pagesEndocrine Disorders: Patho Phys Iolog yCres Padua QuinzonPas encore d'évaluation
- Disorders of Special Senses 2020Document68 pagesDisorders of Special Senses 2020Cres Padua Quinzon100% (1)
- Disorders of Integumentary Function - 2020-2021Document40 pagesDisorders of Integumentary Function - 2020-2021Cres Padua QuinzonPas encore d'évaluation
- Causes and Mechanisms of Acute Renal Injury and Chronic Kidney DiseaseDocument12 pagesCauses and Mechanisms of Acute Renal Injury and Chronic Kidney DiseaseCres Padua QuinzonPas encore d'évaluation
- Musculoskeletal Disorders: Pathophysiology 2020-2021 Oman College of Health Sciences DhofarDocument20 pagesMusculoskeletal Disorders: Pathophysiology 2020-2021 Oman College of Health Sciences DhofarCres Padua QuinzonPas encore d'évaluation
- Disorders of Integrative Function 2 - 2020Document15 pagesDisorders of Integrative Function 2 - 2020Cres Padua QuinzonPas encore d'évaluation
- Disorders of Integumentary Function - 2020-2021 PDFDocument7 pagesDisorders of Integumentary Function - 2020-2021 PDFCres Padua QuinzonPas encore d'évaluation
- Disorders of Integumentary Function - 2020-2021 PDFDocument7 pagesDisorders of Integumentary Function - 2020-2021 PDFCres Padua QuinzonPas encore d'évaluation
- Disorders of Integrative Function 2 - 2020Document15 pagesDisorders of Integrative Function 2 - 2020Cres Padua QuinzonPas encore d'évaluation
- Disorders of The Immune Response and Inflammation 3Document47 pagesDisorders of The Immune Response and Inflammation 3Cres Padua QuinzonPas encore d'évaluation
- AIDSDocument20 pagesAIDSCres Padua QuinzonPas encore d'évaluation
- HUMS111 ResearchDocument8 pagesHUMS111 ResearchCres Padua QuinzonPas encore d'évaluation
- AIDSDocument20 pagesAIDSCres Padua QuinzonPas encore d'évaluation
- Disorders of Respiratory Function - 11Document21 pagesDisorders of Respiratory Function - 11Cres Padua QuinzonPas encore d'évaluation
- Disorders of Blood Pressure Regulation - 10Document31 pagesDisorders of Blood Pressure Regulation - 10Cres Padua QuinzonPas encore d'évaluation
- Case Study Cellular AdaptationDocument1 pageCase Study Cellular AdaptationCres Padua QuinzonPas encore d'évaluation
- Epidural Hematoma, Subdural Hematoma, Meningitis vs Encephalitis, Ischemic vs Hemorrhagic StrokeDocument12 pagesEpidural Hematoma, Subdural Hematoma, Meningitis vs Encephalitis, Ischemic vs Hemorrhagic StrokeCres Padua QuinzonPas encore d'évaluation
- Disorders of Arterial Circulation - 8Document36 pagesDisorders of Arterial Circulation - 8Cres Padua QuinzonPas encore d'évaluation
- Session 5 - Assessment Techniques in Clinical SettingDocument18 pagesSession 5 - Assessment Techniques in Clinical SettingCres Padua QuinzonPas encore d'évaluation
- Gibbs Reflective Journal SampleDocument4 pagesGibbs Reflective Journal SampleCres Padua Quinzon100% (2)
- Disorders of Gastrointestinal FunctionDocument103 pagesDisorders of Gastrointestinal FunctionCres Padua QuinzonPas encore d'évaluation
- Session 4 - Steps of Health AssessmentDocument63 pagesSession 4 - Steps of Health AssessmentCres Padua Quinzon100% (2)
- Gibbs Reflective Journal SampleDocument4 pagesGibbs Reflective Journal SampleCres Padua Quinzon100% (2)
- Disorders of Arterial Circulation - 8Document6 pagesDisorders of Arterial Circulation - 8Cres Padua QuinzonPas encore d'évaluation
- Cultural Beliefs and Values AssessmentDocument19 pagesCultural Beliefs and Values AssessmentCres Padua QuinzonPas encore d'évaluation
- Cultural Beliefs and Values AssessmentDocument19 pagesCultural Beliefs and Values AssessmentCres Padua QuinzonPas encore d'évaluation
- Pancreatitis Ishikawa 2016Document19 pagesPancreatitis Ishikawa 2016Limbert RodriguezPas encore d'évaluation
- HC776Document4 pagesHC776Dawn CasuncadPas encore d'évaluation
- The Differences Between Coaching Mentoring Therapy and Counselling PDFDocument5 pagesThe Differences Between Coaching Mentoring Therapy and Counselling PDFghinaPas encore d'évaluation
- Intestinal DisordersDocument11 pagesIntestinal DisorderspulmonologistPas encore d'évaluation
- How To Silence Fear and Win The Mental Game: Companion WorkbookDocument55 pagesHow To Silence Fear and Win The Mental Game: Companion WorkbookMayur Merchant89% (9)
- Oral Candidiasis: Dr. Ahmad Yusran, SPPDDocument87 pagesOral Candidiasis: Dr. Ahmad Yusran, SPPDM Nedi Sevtia BudiPas encore d'évaluation
- S - "Sakit Ahong Tinahian" As Verbalized byDocument6 pagesS - "Sakit Ahong Tinahian" As Verbalized bylandilinoPas encore d'évaluation
- Managerial accounting report on Homestead family clinic case studyDocument19 pagesManagerial accounting report on Homestead family clinic case studyIbrahim AmmarPas encore d'évaluation
- Better Living With COPDDocument108 pagesBetter Living With COPDPrem AnandPas encore d'évaluation
- Preterm Labor ManagementDocument50 pagesPreterm Labor ManagementDr-Firas Nayf Al-ThawabiaPas encore d'évaluation
- Nursing Process and Clinical Reasoning Cycle GuideDocument8 pagesNursing Process and Clinical Reasoning Cycle GuideTijanne-Jayde CunialPas encore d'évaluation
- Mental Health Nursing RequirementsDocument5 pagesMental Health Nursing RequirementsNuay LaoPas encore d'évaluation
- Psychological First Aid-A Training GuideDocument8 pagesPsychological First Aid-A Training Guidejprewittdiaz100% (1)
- RICE or MEAT Protocol For Acute Ligament Sprain Treatment - The Sports PhysiotherapistDocument4 pagesRICE or MEAT Protocol For Acute Ligament Sprain Treatment - The Sports PhysiotherapistZach FallonPas encore d'évaluation
- ImhDocument12 pagesImhMimi Lizada BhattiPas encore d'évaluation
- Drug StudyDocument4 pagesDrug Studymisstheatricality130Pas encore d'évaluation
- Patellofemoral Final PDFDocument12 pagesPatellofemoral Final PDFdvenumohanPas encore d'évaluation
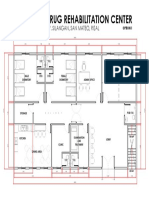
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDocument1 pageProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonPas encore d'évaluation
- Ana de Castro ResumeDocument1 pageAna de Castro Resumeapi-251818080Pas encore d'évaluation
- InlayDocument33 pagesInlayJitender Reddy75% (4)
- Pharmacology of Interferons: Mechanisms, Indications, and Treatment of Hepatitis CDocument30 pagesPharmacology of Interferons: Mechanisms, Indications, and Treatment of Hepatitis CRam NareshPas encore d'évaluation
- Accidental Intravenous Infusion of Air: A Concise ReviewDocument5 pagesAccidental Intravenous Infusion of Air: A Concise ReviewSiswand BIn Mohd AliPas encore d'évaluation
- Revista Chilena de Neuro-Psiquiatría: La Persona Del Terapeuta: Eje Fundamental de Todo Proceso TerapéuticoDocument13 pagesRevista Chilena de Neuro-Psiquiatría: La Persona Del Terapeuta: Eje Fundamental de Todo Proceso TerapéuticocysagasPas encore d'évaluation
- Cervical Cancer (ECC)Document14 pagesCervical Cancer (ECC)Legi VamelaPas encore d'évaluation
- What Are Extrapyramidal SymptomsDocument2 pagesWhat Are Extrapyramidal SymptomscristieristiiePas encore d'évaluation
- Diuretic DrugsDocument16 pagesDiuretic DrugslabillabooPas encore d'évaluation
- Healing Landscapes: Gardens As Places For Spiritual, Psychological and Physical HealingDocument49 pagesHealing Landscapes: Gardens As Places For Spiritual, Psychological and Physical HealingrajshreePas encore d'évaluation
- Catholic Teaching on Gender Dysphoria and TreatmentDocument23 pagesCatholic Teaching on Gender Dysphoria and TreatmentAntónio AlvimPas encore d'évaluation
- Magic of TouchDocument28 pagesMagic of TouchkurniawatiPas encore d'évaluation
- 81 - Review of The Clinical Efficacy of Traumeel PDFDocument14 pages81 - Review of The Clinical Efficacy of Traumeel PDFmdkkavathekarPas encore d'évaluation