Vous aimerez peut-être aussi
- MedSurg NeuroDocument8 pagesMedSurg NeuroZachary T Hall100% (1)
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideD'EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuidePas encore d'évaluation
- Neurology Nursing Study GuideDocument19 pagesNeurology Nursing Study GuideHayleyLangley100% (5)
- Medical-Surgical Nursing Exam 18 - Neurological Disorders (34 Items) - NurseslabsDocument7 pagesMedical-Surgical Nursing Exam 18 - Neurological Disorders (34 Items) - NurseslabsRandySandoval100% (1)
- Chapter 66 - Management of Patients With Neurologic DysfunctionDocument54 pagesChapter 66 - Management of Patients With Neurologic DysfunctionFeliciaDorgham100% (2)
- Chapter 68 - Management of Patients With Neurologic TraumaDocument49 pagesChapter 68 - Management of Patients With Neurologic TraumaFeliciaDorghamPas encore d'évaluation
- Increased Intracranial PressureDocument17 pagesIncreased Intracranial Pressureapi-232466940100% (1)
- Medical Surgical Nursing Reviewer BulletsDocument8 pagesMedical Surgical Nursing Reviewer Bulletsgrey26100% (3)
- Nursing Lecture NeurologicalDocument28 pagesNursing Lecture NeurologicalAedge010100% (1)
- Medical Surgical Nursing Cardio Vascular System ClassDocument15 pagesMedical Surgical Nursing Cardio Vascular System Classvallal100% (2)
- Chapter60 Assessment of Neurologic FunctionDocument25 pagesChapter60 Assessment of Neurologic FunctionAhmed 123Pas encore d'évaluation
- Head Injury Causes and TreatmentDocument47 pagesHead Injury Causes and TreatmentnikowarePas encore d'évaluation
- Mabes Fluid and Electrolyte ImbalancesDocument15 pagesMabes Fluid and Electrolyte ImbalancesMabesPas encore d'évaluation
- Medical Surgical Nursing Common Drugs and Its AntidotesDocument2 pagesMedical Surgical Nursing Common Drugs and Its AntidotesJhannPas encore d'évaluation
- Emergency NursingDocument19 pagesEmergency Nursingshenric16Pas encore d'évaluation
- Patients With Hearing and Balance DisordersDocument33 pagesPatients With Hearing and Balance Disordershalloween candyPas encore d'évaluation
- Seizure PathophysiologyDocument2 pagesSeizure PathophysiologyqwertyuiopPas encore d'évaluation
- Nursing care of musculoskeletal disorders in childrenDocument180 pagesNursing care of musculoskeletal disorders in childrenRiccyPas encore d'évaluation
- Eyes and EarsDocument17 pagesEyes and Earsdlneisha61100% (2)
- Intracranial HemorrhageDocument41 pagesIntracranial Hemorrhagedoctormussieaberra100% (1)
- Gerontologic Health Promotion ActivityDocument3 pagesGerontologic Health Promotion ActivityCorinne50% (2)
- Acute Respiratory Distress SyndromeDocument31 pagesAcute Respiratory Distress Syndromegretchen marie100% (1)
- Central Venous Pressure MonitoringDocument2 pagesCentral Venous Pressure MonitoringpauchanmnlPas encore d'évaluation
- Encephalitis PathophysiologyDocument19 pagesEncephalitis PathophysiologyHeron Bayanin80% (5)
- Neurologic NursingDocument14 pagesNeurologic Nursingtheglobalnursing100% (6)
- Hematologic System and DisordersDocument68 pagesHematologic System and DisordersRellie Castro100% (1)
- Compilation of MS NotesDocument81 pagesCompilation of MS Notesdis_is_mePas encore d'évaluation
- Assessment and Management of Patients With Endocrine DisordersDocument11 pagesAssessment and Management of Patients With Endocrine DisordersLesley GonzalezPas encore d'évaluation
- Factors That Cause Epilepsy & Signs of SeizuresDocument2 pagesFactors That Cause Epilepsy & Signs of SeizuresAnjelika Eurelle Caliboso Mapili100% (1)
- Anaphylactic Shock Nursing NotesDocument6 pagesAnaphylactic Shock Nursing Notesjtlammers100% (1)
- Med-Surg Nusing BulletsDocument65 pagesMed-Surg Nusing BulletsHarley C. Tan100% (1)
- Chart of Neuro DisordersDocument1 pageChart of Neuro DisordersNursingSchoolNotes100% (2)
- Perception and CoordinationDocument32 pagesPerception and CoordinationFerdie Marcial B. AureaPas encore d'évaluation
- PPPDocument3 pagesPPPJack BangcoyoPas encore d'évaluation
- Fluids & Electrolyte NewDocument154 pagesFluids & Electrolyte NewMaria Visitacion100% (2)
- Nursing Care PlanDocument6 pagesNursing Care Planesteffie21Pas encore d'évaluation
- Med SurgDocument98 pagesMed SurgKimsha Concepcion88% (8)
- Physical AssessmentDocument12 pagesPhysical Assessmentteslimolakunleraji100% (1)
- Heart Failure Case StudyDocument2 pagesHeart Failure Case StudyRC0% (1)
- Altered Level of ConsciousnessDocument11 pagesAltered Level of ConsciousnessRamji PaudelPas encore d'évaluation
- Meningocele Case Study (Emergency Nursing) - Theory BasedDocument47 pagesMeningocele Case Study (Emergency Nursing) - Theory BasedKyssel Seyer100% (2)
- ARDS MANAGEMENT GUIDEDocument2 pagesARDS MANAGEMENT GUIDETisha CarrettePas encore d'évaluation
- Burn PPT CH 62Document47 pagesBurn PPT CH 62ضياء عمارنه50% (2)
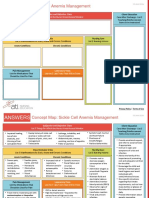
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDocument2 pagesNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- Psychiatric Nursing NotesDocument13 pagesPsychiatric Nursing NotesCarlo VigoPas encore d'évaluation
- Pediatric Nursing Pediatric NursingDocument59 pagesPediatric Nursing Pediatric Nursingmaj100% (2)
- Neurological Disorders - SIMCLEXDocument10 pagesNeurological Disorders - SIMCLEXLLLJJJPas encore d'évaluation
- EENTDocument52 pagesEENTdr2tin100% (1)
- Cardiac Tamponade 2Document23 pagesCardiac Tamponade 2Jethro Floyd QuintoPas encore d'évaluation
- Assessment and Management of Patients With Hearing and Balance Disorders WebDocument36 pagesAssessment and Management of Patients With Hearing and Balance Disorders WebStephKirstin Velasco Malapit100% (2)
- Nursing Management of Patient With CCFDocument34 pagesNursing Management of Patient With CCFJayarani Ashok100% (1)
- Nursing case study on EncephalitisDocument7 pagesNursing case study on EncephalitisJitendraPas encore d'évaluation
- Brain AbscessDocument5 pagesBrain AbscessEugene Briagas Roque100% (1)
- Neuro Study GuideDocument7 pagesNeuro Study GuideNursingSchoolNotes100% (2)
- II-E Altered PerceptionDocument16 pagesII-E Altered PerceptionDharylle CariñoPas encore d'évaluation
- Organic Mental Disorder: Presented By: Priyanka Kumari M.Sc. NursingDocument50 pagesOrganic Mental Disorder: Presented By: Priyanka Kumari M.Sc. NursingHardeep KaurPas encore d'évaluation
- Chapter 14 Neurologic Disorders Study Guide Outline #2Document12 pagesChapter 14 Neurologic Disorders Study Guide Outline #2Del Delgado100% (1)
- Ischemic Stroke - 3B5Document77 pagesIschemic Stroke - 3B5Aireen Grace GilosPas encore d'évaluation
- How To Make Neurological Diagnosis NewDocument34 pagesHow To Make Neurological Diagnosis NewPeter AsaPas encore d'évaluation
- Chapter Three: Understanding Your Communication StyleDocument76 pagesChapter Three: Understanding Your Communication StyleSapiah RamanPas encore d'évaluation
- Ssessment Remediation 1Document6 pagesSsessment Remediation 1Sapiah RamanPas encore d'évaluation
- Nursing ProcessDocument55 pagesNursing ProcessSapiah Raman100% (1)
- Occupational Health Nursing RoleDocument48 pagesOccupational Health Nursing RoleSapiah Raman50% (4)
- Nursing ProcessDocument55 pagesNursing ProcessSapiah Raman100% (1)
- Community Health NursingDocument237 pagesCommunity Health Nursingjhing_apdan100% (2)
- Dip Nursing Aide 11Document26 pagesDip Nursing Aide 11Sapiah RamanPas encore d'évaluation
- Kingdom of Saudi Arabia King Fahd Hospital Jeddah: Intensive Care UnitDocument41 pagesKingdom of Saudi Arabia King Fahd Hospital Jeddah: Intensive Care UnitSapiah RamanPas encore d'évaluation
- Chap 003Document24 pagesChap 003Sapiah Raman100% (1)
- CHNDocument136 pagesCHNSapiah RamanPas encore d'évaluation
- Management C05 Decision Making WebDocument5 pagesManagement C05 Decision Making WebSapiah RamanPas encore d'évaluation
- ICU Admission PolicyDocument4 pagesICU Admission PolicySapiah RamanPas encore d'évaluation
- Community Health Nursing Examination Part IDocument17 pagesCommunity Health Nursing Examination Part Iɹǝʍdןnos97% (64)
- Chapter 1Document31 pagesChapter 1Sapiah Raman100% (1)
- 1 2carbohydrates 120607083032 Phpapp02Document48 pages1 2carbohydrates 120607083032 Phpapp02Sapiah RamanPas encore d'évaluation
- NUTRITIONDocument35 pagesNUTRITIONSapiah RamanPas encore d'évaluation
- The Malaysian Vision 2020 That Was Embarked in 1991Document4 pagesThe Malaysian Vision 2020 That Was Embarked in 1991Sapiah RamanPas encore d'évaluation
- MODULE 1: Critical Thinking in Nursing Practice and Nursing ProcessDocument5 pagesMODULE 1: Critical Thinking in Nursing Practice and Nursing ProcessSapiah RamanPas encore d'évaluation
- Case Study # 3 UNRS 314 Name - Number - Ruptured AppendixDocument2 pagesCase Study # 3 UNRS 314 Name - Number - Ruptured AppendixSapiah RamanPas encore d'évaluation
- Thesis 3Document9 pagesThesis 3Yuvaraj KrishnanPas encore d'évaluation
- Antibiotics:: Sulfonamides Penicillins Cephalosporins Tetracyclines Aminoglycosides Quinolones MacrolidesDocument67 pagesAntibiotics:: Sulfonamides Penicillins Cephalosporins Tetracyclines Aminoglycosides Quinolones MacrolidesMarcky_467100% (7)
- Islamic Philosophy and History of EducationDocument18 pagesIslamic Philosophy and History of EducationSapiah RamanPas encore d'évaluation
- 1134 - jp-v10n2 - Planning An Affective Education For Pre-School Children - Within Islamic and Western Perspective - Mastura BadzisDocument14 pages1134 - jp-v10n2 - Planning An Affective Education For Pre-School Children - Within Islamic and Western Perspective - Mastura BadzisSapiah RamanPas encore d'évaluation
- Management TheoryDocument15 pagesManagement TheorySapiah RamanPas encore d'évaluation
- Care of The Controlled SubstancesDocument32 pagesCare of The Controlled SubstancesSapiah Raman0% (1)
- Introduction To HaemostasisDocument18 pagesIntroduction To Haemostasiswatchme3Pas encore d'évaluation
- General: - Cranial Nerves Same As Spinal ButDocument5 pagesGeneral: - Cranial Nerves Same As Spinal ButjPas encore d'évaluation
- Male Genitals and Inguinal AreaDocument33 pagesMale Genitals and Inguinal AreabianqueePas encore d'évaluation
- Learning Activity Sheet Grade 10 Science: Feedback Mechanisms: Key To HomeostasisDocument4 pagesLearning Activity Sheet Grade 10 Science: Feedback Mechanisms: Key To HomeostasisKeisha Janelle ZetazatePas encore d'évaluation
- LPDocument3 pagesLPRovelyn ClementePas encore d'évaluation
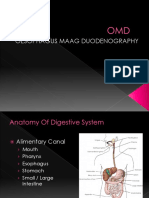
- Oesophagus Maag DuodenographyDocument49 pagesOesophagus Maag DuodenographyEvan DionesiaPas encore d'évaluation
- Curs5 Hematologie AnvDocument59 pagesCurs5 Hematologie AnvRaluca PăunaPas encore d'évaluation
- Understanding Joints and ArticulationsDocument26 pagesUnderstanding Joints and Articulationsragnarok meroPas encore d'évaluation
- BloodDocument17 pagesBloodfatimamuzammil406Pas encore d'évaluation
- Osce AbdomenDocument33 pagesOsce AbdomenistiPas encore d'évaluation
- Zachary A. Riley, Stéphane Baudry and Roger M. Enoka: This Article CitesDocument10 pagesZachary A. Riley, Stéphane Baudry and Roger M. Enoka: This Article Citesrizki yulita rahmahPas encore d'évaluation
- (K4) Male Reproductive SystemDocument73 pages(K4) Male Reproductive SystemJane Andrea Christiano DjianzoniePas encore d'évaluation
- Principles of Renal Physiology: Fifth EditionDocument15 pagesPrinciples of Renal Physiology: Fifth EditionAISHAPas encore d'évaluation
- Neurofunctional Blueprints Transcripts For Tempe, January 2015 PDFDocument82 pagesNeurofunctional Blueprints Transcripts For Tempe, January 2015 PDFAnonymous oCjRxyBP100% (3)
- Ubogu - Inflammatory NeuropathiesDocument24 pagesUbogu - Inflammatory NeuropathiesMarcelo BedoyaPas encore d'évaluation
- CVD Q's & A'sDocument9 pagesCVD Q's & A'sAlan TaylorPas encore d'évaluation
- 320401409mary Princes Sulekha PDFDocument140 pages320401409mary Princes Sulekha PDFAnand RasPas encore d'évaluation
- NeuroDocument317 pagesNeuroNela Popa100% (2)
- Zoology Notes on Physiology, Anatomy and GeneticsDocument11 pagesZoology Notes on Physiology, Anatomy and GeneticskrishnaPas encore d'évaluation
- Trans Chapter 16Document5 pagesTrans Chapter 16رجمه ديوانPas encore d'évaluation
- Blood Vessels QuestionsDocument7 pagesBlood Vessels QuestionsT-Jay Ellis-DalePas encore d'évaluation
- The Anatomy of The Tooth WORKSHEETDocument4 pagesThe Anatomy of The Tooth WORKSHEETAndaPas encore d'évaluation
- Mechanisms of Coagulation and Fibrinolysis (Autosaved)Document60 pagesMechanisms of Coagulation and Fibrinolysis (Autosaved)Tom Anthony TonguiaPas encore d'évaluation
- Absen Pembacaan Refarat Dan Lapsus Suci RamadhaniDocument2 pagesAbsen Pembacaan Refarat Dan Lapsus Suci Ramadhanisuci ramadhaniPas encore d'évaluation
- Anatomy and Pathophysiology of AnemiaDocument9 pagesAnatomy and Pathophysiology of AnemiaDarlen Rabano88% (8)
- Chronic Hyperplastic PulpitisDocument30 pagesChronic Hyperplastic PulpitisGlory Pohan67% (3)
- Heart Anatomy Diagram Error: Atria LabelsDocument2 pagesHeart Anatomy Diagram Error: Atria LabelskayannaPas encore d'évaluation
- Seven Plus One Lymph HealingDocument3 pagesSeven Plus One Lymph HealingAnonymous hndaj8zCA50% (2)
- Ch11 Lecture PPT ADocument66 pagesCh11 Lecture PPT AMiky rose De GuzmanPas encore d'évaluation
- #3 Balance of Liquid and Electrolite in Animal BodyDocument13 pages#3 Balance of Liquid and Electrolite in Animal BodyYodi MainantoPas encore d'évaluation