Vous aimerez peut-être aussi
- Ovarian Torsion: Angie Child, Harvard Medical School IV Gillian Lieberman, MDDocument27 pagesOvarian Torsion: Angie Child, Harvard Medical School IV Gillian Lieberman, MDNishchay TripathiPas encore d'évaluation
- Plante-2016-Management of Sepsis and Septic Shock For The Obstetrician-Gynecologist PDFDocument20 pagesPlante-2016-Management of Sepsis and Septic Shock For The Obstetrician-Gynecologist PDFntnquynhproPas encore d'évaluation
- IDSA Bacteriuria AsintomaticaDocument12 pagesIDSA Bacteriuria AsintomaticaAriadna_PattyPas encore d'évaluation
- Borderline Mucinous Ovarian Tumor Presenting As Pseudo Meigs SyndromeDocument4 pagesBorderline Mucinous Ovarian Tumor Presenting As Pseudo Meigs SyndromeJulie MayPas encore d'évaluation
- Imaging of Acute Abdomen in PregnancyDocument18 pagesImaging of Acute Abdomen in Pregnancyshofa nur rahmannisaPas encore d'évaluation
- Burlinson-2018-Sepsis in Pregnancy and The Puerperium PDFDocument12 pagesBurlinson-2018-Sepsis in Pregnancy and The Puerperium PDFntnquynhproPas encore d'évaluation
- Ovarian Torsion After Ovarian Hyperstimulation SyndromeDocument2 pagesOvarian Torsion After Ovarian Hyperstimulation SyndromeasclepiuspdfsPas encore d'évaluation
- Defining and Diagnosing SepsisDocument9 pagesDefining and Diagnosing SepsisEdwin AlvarezPas encore d'évaluation
- Ovarian TorsiDocument8 pagesOvarian TorsiSebastian GandyPas encore d'évaluation
- Lapsus Susp - Ca EndometriumDocument22 pagesLapsus Susp - Ca Endometriumjeams manuPas encore d'évaluation
- Acute Abdominal Pain in Pregnancy: Diagnosis and Management Conservative vs. SurgicalDocument73 pagesAcute Abdominal Pain in Pregnancy: Diagnosis and Management Conservative vs. SurgicalIgnatov OanaPas encore d'évaluation
- Urogenital Infections Linked to Preterm LaborDocument4 pagesUrogenital Infections Linked to Preterm LaborPangalanitaPas encore d'évaluation
- Hemorragic CystDocument14 pagesHemorragic CystNyoman TapayanaPas encore d'évaluation
- Acute Urinary Retention: Ronald TanggoDocument63 pagesAcute Urinary Retention: Ronald TanggoKalista ApriyaniPas encore d'évaluation
- Assessment of The Medical PatientDocument84 pagesAssessment of The Medical PatientbrentupdegraffPas encore d'évaluation
- Estimating Postmortem Interval Using Accumulated Degree Days and A Degree of DecDocument21 pagesEstimating Postmortem Interval Using Accumulated Degree Days and A Degree of DecRahma MaharsiPas encore d'évaluation
- IV Access and Medication AdministrationDocument47 pagesIV Access and Medication AdministrationbrentupdegraffPas encore d'évaluation
- Referat RahmanDocument27 pagesReferat Rahmannasution7Pas encore d'évaluation
- Guildelines For Hiv Testing NacoDocument165 pagesGuildelines For Hiv Testing NacoNagendra Singh BeniwalPas encore d'évaluation
- Paracervical block technique and complicationsDocument4 pagesParacervical block technique and complicationspolygonePas encore d'évaluation
- Etiologi Dan Patogenesis Kondiloma Akuminatum-Kelompok 3Document16 pagesEtiologi Dan Patogenesis Kondiloma Akuminatum-Kelompok 3Nitha SarinaPas encore d'évaluation
- Dr. Kruvilla - Hyperthyroidism in PregnancyDocument38 pagesDr. Kruvilla - Hyperthyroidism in PregnancyjarvantaraPas encore d'évaluation
- Batu PyelumDocument29 pagesBatu PyelumDanniel KamarudinPas encore d'évaluation
- Pelvic Inflammatory Disease: Dr. Indah Meyliza, M. KesDocument13 pagesPelvic Inflammatory Disease: Dr. Indah Meyliza, M. KesIndah MeylizaPas encore d'évaluation
- Therapeutic Guidelines Antimicrobial Prophylaxis SurgeryDocument86 pagesTherapeutic Guidelines Antimicrobial Prophylaxis SurgeryhendryfransiskusPas encore d'évaluation
- Referat Muhammad Aris IndrawanDocument41 pagesReferat Muhammad Aris IndrawanridhaPas encore d'évaluation
- Woman with Vesicovaginal, Ureterocutaneous and Ureterorectal FistulaeDocument24 pagesWoman with Vesicovaginal, Ureterocutaneous and Ureterorectal Fistulaemizz_jcPas encore d'évaluation
- Demam Tipoid: Divisi Infeksi Dan Penyakit Tropis Departemen Ilmu Kesehatan Anak FK UNDIP/RSUP Dr. Kariadi Semarang 2015Document50 pagesDemam Tipoid: Divisi Infeksi Dan Penyakit Tropis Departemen Ilmu Kesehatan Anak FK UNDIP/RSUP Dr. Kariadi Semarang 2015Andri Tri AtmojoPas encore d'évaluation
- Evaluation of PupilDocument28 pagesEvaluation of PupilArlinda Silva PrameswariPas encore d'évaluation
- Lesi Osteolitic Costa 6 Belakang S Lesi Osteoblastic Costa 6-7 Belakang DDocument48 pagesLesi Osteolitic Costa 6 Belakang S Lesi Osteoblastic Costa 6-7 Belakang DLusi MunawarohPas encore d'évaluation
- Hemorrhage - ShockDocument55 pagesHemorrhage - Shocktusharbk08313100% (2)
- Pleno Skenario A Blok 23Document24 pagesPleno Skenario A Blok 23Imam Adli MuhammadPas encore d'évaluation
- Diagnosing and Treating Tuberculosis MeningitisDocument6 pagesDiagnosing and Treating Tuberculosis MeningitisGarrett SimpsonPas encore d'évaluation
- Seboroik DermatitisDocument21 pagesSeboroik DermatitisPutri PelealuPas encore d'évaluation
- Optimizing Monotherapy of Colicky Abdominal PainDocument31 pagesOptimizing Monotherapy of Colicky Abdominal PainRahmad AjahPas encore d'évaluation
- Advancement in Partograph WHO's Labor Care GuideDocument7 pagesAdvancement in Partograph WHO's Labor Care GuideSujan ThapaPas encore d'évaluation
- 13 - 266fourniers Gangrene PDFDocument5 pages13 - 266fourniers Gangrene PDFMochamad RizalPas encore d'évaluation
- Pemakaian Antibiotik Polifarmasi Pada GeritariDocument37 pagesPemakaian Antibiotik Polifarmasi Pada GeritariShinta LissevaPas encore d'évaluation
- Surg PPX GuidelineDocument38 pagesSurg PPX Guidelinefarah azizahPas encore d'évaluation
- Tatalaksana Anestesi Untuk Appendiktomi Pada Pasien AppendisitisDocument34 pagesTatalaksana Anestesi Untuk Appendiktomi Pada Pasien AppendisitisIdha FitriyaniPas encore d'évaluation
- Shoulder Dystocia GuideDocument66 pagesShoulder Dystocia GuidesteffiesolinPas encore d'évaluation
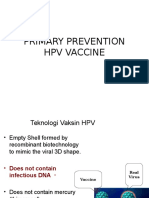
- Vaksin HPVDocument14 pagesVaksin HPVsutianiPas encore d'évaluation
- Tutorial Kasus: AppendisitisDocument50 pagesTutorial Kasus: Appendisitiseruza hiwatariPas encore d'évaluation
- What Is New in The Treatment of SepsisDocument49 pagesWhat Is New in The Treatment of SepsisOlga GoryachevaPas encore d'évaluation
- Persalinan NormalDocument26 pagesPersalinan NormalAnasZakariaPas encore d'évaluation
- 2022 ESHRE RPL Guideline Update 2022 Draft For Stakeholder ReviewDocument157 pages2022 ESHRE RPL Guideline Update 2022 Draft For Stakeholder ReviewDairo PintoPas encore d'évaluation
- Case SirosisDocument19 pagesCase SirosisZehna NzPas encore d'évaluation
- Antibiotic Prescribing: How Can Emergence of Antibiotic Resistance Be Delayed?Document4 pagesAntibiotic Prescribing: How Can Emergence of Antibiotic Resistance Be Delayed?Marak EnPas encore d'évaluation
- 1 Anatomi Organ PanggulDocument45 pages1 Anatomi Organ PanggulHutomo Budi Hasnian SyahPas encore d'évaluation
- Efektivitas Antibiotik Pada Kaki DiabetikDocument6 pagesEfektivitas Antibiotik Pada Kaki DiabetikFawzia Haznah Nurul ImaniPas encore d'évaluation
- Referat Meningitis AnakDocument24 pagesReferat Meningitis AnakSyarifah Maharani HidayatPas encore d'évaluation
- Journal Reading GastroschisisDocument36 pagesJournal Reading GastroschisisShindi Yunia PurwantoPas encore d'évaluation
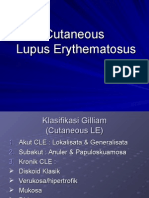
- Cutaneous Lupus ErythematosusDocument15 pagesCutaneous Lupus ErythematosusErika KusumawatiPas encore d'évaluation
- Current Concepts in The Pathogenesis and Treatment of Chronic Suppurative Otitis MediaDocument31 pagesCurrent Concepts in The Pathogenesis and Treatment of Chronic Suppurative Otitis Mediafurqon alPas encore d'évaluation
- OB 1.06A History Taking, Diagnosis, and Pre-Natal CareDocument21 pagesOB 1.06A History Taking, Diagnosis, and Pre-Natal CareCandice SongcoPas encore d'évaluation
- Hemorragic Post PartumDocument35 pagesHemorragic Post PartumMuhammad AsrizalPas encore d'évaluation
- Diagnosis & Penanganan Syok HemoragDocument31 pagesDiagnosis & Penanganan Syok HemoragRidwan RahmanPas encore d'évaluation
- Perioperative Fluid TherapyDocument36 pagesPerioperative Fluid TherapyUmhy GumianaPas encore d'évaluation
- Acute Trauma Care:: ShockDocument45 pagesAcute Trauma Care:: ShockGeoffrey100% (1)
- SHOCKDocument60 pagesSHOCKJoseph John K PothanikatPas encore d'évaluation
- Deadly Lockjaw Disease: Symptoms and Causes of TetanusDocument9 pagesDeadly Lockjaw Disease: Symptoms and Causes of TetanusRiz Sanfebrian AdiatmaPas encore d'évaluation
- Manajemen Perforasi GasterDocument21 pagesManajemen Perforasi GasterRosfi Firdha HuzaimaPas encore d'évaluation
- Periappendicular InfiltrateDocument5 pagesPeriappendicular InfiltrateRiz Sanfebrian AdiatmaPas encore d'évaluation
- Daftar PustakaDocument1 pageDaftar Pustakanouval_iqbalPas encore d'évaluation
- Data Internship 52Document1 pageData Internship 52Riz Sanfebrian AdiatmaPas encore d'évaluation
- Halohaaaa Halohaa HalohaaaaDocument1 pageHalohaaaa Halohaa HalohaaaaRiz Sanfebrian AdiatmaPas encore d'évaluation
- Daftar PustakaDocument1 pageDaftar Pustakanouval_iqbalPas encore d'évaluation
- Follow Up TN MasnorDocument6 pagesFollow Up TN MasnorRiz Sanfebrian AdiatmaPas encore d'évaluation
- Ginasthma.orgDocument30 pagesGinasthma.orgRoberto BPPas encore d'évaluation
- GFWLIVESetup Log VerboseDocument1 pageGFWLIVESetup Log VerboseAlejandro PiñeiroPas encore d'évaluation
- GFWLIVESetup LogDocument1 pageGFWLIVESetup LogMorten MidtkandalPas encore d'évaluation
- Nclex Study GuideDocument35 pagesNclex Study Guideapi-238869635100% (3)
- Introduction To Maritime Safety Complete ModuleDocument46 pagesIntroduction To Maritime Safety Complete ModuleHarold Navares Jr.100% (4)
- EFA - Module 2 r1Document57 pagesEFA - Module 2 r1Jerry CañeroPas encore d'évaluation
- Shock Types and Management in ObstetricsDocument25 pagesShock Types and Management in ObstetricsNinaPas encore d'évaluation
- Emergency Medicine EbookDocument642 pagesEmergency Medicine Ebookgulsoomro100% (1)
- Shock: Robert H. Sirait, DR.,SP An Dept. of Anesthesia FK UKI JakartaDocument22 pagesShock: Robert H. Sirait, DR.,SP An Dept. of Anesthesia FK UKI JakartaMuhammad Faisal AminPas encore d'évaluation
- Shock HypovolemicDocument16 pagesShock HypovolemicTitinPas encore d'évaluation
- FebruaryDocument56 pagesFebruarypehuyPas encore d'évaluation
- Physiology Summary Chapter 20Document9 pagesPhysiology Summary Chapter 20gail01850% (2)
- Elementary First Aid Power Point (Efa) - oRIGINALDocument183 pagesElementary First Aid Power Point (Efa) - oRIGINALClark Llamera100% (1)
- First AidDocument54 pagesFirst AidMadhavi ModaPas encore d'évaluation
- 50 Multiple ChoiceDocument11 pages50 Multiple ChoiceMac Chi Le Nu83% (6)
- Fluid Management in Dengue Hemorrhagic FeverDocument38 pagesFluid Management in Dengue Hemorrhagic FeverMarvin OcampoPas encore d'évaluation
- Levy2018 Surviving Sepsis Camapign 2018Document8 pagesLevy2018 Surviving Sepsis Camapign 2018ronie redsPas encore d'évaluation
- Pediatric AssessmentDocument16 pagesPediatric AssessmentWenTzu100% (2)
- Anaphylaxis Reaction & Drug Allergy 2Document47 pagesAnaphylaxis Reaction & Drug Allergy 2telusurPas encore d'évaluation
- News & Views: Restrictive Fluid Therapy and High-Dose Vitamin C in SepsisDocument2 pagesNews & Views: Restrictive Fluid Therapy and High-Dose Vitamin C in SepsisLAURA ALEJANDRA GONZALEZ MONTOYAPas encore d'évaluation
- Advance Trauma Life SupportDocument67 pagesAdvance Trauma Life SupportraffellaPas encore d'évaluation
- Pathophysiology, Monitoring, and Therapy of Shock With Organ FailureDocument11 pagesPathophysiology, Monitoring, and Therapy of Shock With Organ FailureAli SedawiPas encore d'évaluation
- The Acute Hemoabdomen: Topic OverviewDocument23 pagesThe Acute Hemoabdomen: Topic OverviewWeiwei CierraPas encore d'évaluation
- Shock Case StudyDocument2 pagesShock Case StudyDonna LLerandiPas encore d'évaluation
- CTC Lecture NotesDocument28 pagesCTC Lecture NotesAda WongPas encore d'évaluation
- BleedingDocument72 pagesBleedingRHENCE TEJEROPas encore d'évaluation
- Maternal and Child Nursing - Postpartum CareDocument54 pagesMaternal and Child Nursing - Postpartum Carechuppepay33% (3)
- Exam First-AidDocument5 pagesExam First-AidMarielle Rumbaoa0% (1)
- Thesis Bone Tissue EngineeringDocument6 pagesThesis Bone Tissue Engineeringsarahturnerdesmoines100% (2)
- BEC Post-Test Answer Key 2Document1 pageBEC Post-Test Answer Key 2zinabuhaile26Pas encore d'évaluation
- Pediatric Hospital Care Ethiopia - 2016Document526 pagesPediatric Hospital Care Ethiopia - 2016Tony Tefera100% (3)
- Medicine - I T&D DECEMBER - 2021 Paper Discussion: DR Deepak MarwahDocument84 pagesMedicine - I T&D DECEMBER - 2021 Paper Discussion: DR Deepak MarwahHafuz DodiyaPas encore d'évaluation
- Nursing Diagnosis and Nursing Interventions For Dengue Hemorrhagic FeverDocument2 pagesNursing Diagnosis and Nursing Interventions For Dengue Hemorrhagic FeverThirdy Aquino82% (28)