Vous aimerez peut-être aussi
- Abdominal ParacentesisDocument5 pagesAbdominal Paracentesisw wPas encore d'évaluation
- Peritoneal DialysisDocument10 pagesPeritoneal DialysisPdianghunPas encore d'évaluation
- Rules and Directions for the Employment of Injections in Various DiseasesD'EverandRules and Directions for the Employment of Injections in Various DiseasesPas encore d'évaluation
- Abdominal Paracentesis AnpDocument14 pagesAbdominal Paracentesis Anpesther100% (1)
- Diverticulitis Cure: The Ultimate Diverticulitis Diet: Diverticulitis Recipes: Your Ultimate Diverticulitis CookbookD'EverandDiverticulitis Cure: The Ultimate Diverticulitis Diet: Diverticulitis Recipes: Your Ultimate Diverticulitis CookbookPas encore d'évaluation
- Common Procedures in Paediatric IcuDocument17 pagesCommon Procedures in Paediatric IcuNeethu Mariya MathewPas encore d'évaluation
- Abdominal Paracentesis.Document4 pagesAbdominal Paracentesis.Sukh Preet100% (1)
- Abdominal ParacentesisDocument5 pagesAbdominal ParacentesisSivaprasad S100% (1)
- Chapter VDocument15 pagesChapter VJellou MacPas encore d'évaluation
- Peritoneal DialysisDocument29 pagesPeritoneal DialysisMicah Alexis CandelarioPas encore d'évaluation
- Assignment On Abdominal ParacentesisDocument9 pagesAssignment On Abdominal ParacentesisAxsa AlexPas encore d'évaluation
- Blood Transfusion: Nursing ProcedureDocument52 pagesBlood Transfusion: Nursing ProcedureAlessandro Ivan MiguelPas encore d'évaluation
- Peritoneal LavageDocument30 pagesPeritoneal Lavageapi-3722454100% (2)
- Acs NotesDocument5 pagesAcs NotesRheaPas encore d'évaluation
- Peritoneal DialysisDocument31 pagesPeritoneal Dialysisapi-372245489% (9)
- Abdominal ParasynthesisDocument5 pagesAbdominal ParasynthesisLakshmi RjPas encore d'évaluation
- PARACENTESISDocument15 pagesPARACENTESISSoonh ChannaPas encore d'évaluation
- Nursing Management of Patient Undergoing Peritoneal DialysisDocument27 pagesNursing Management of Patient Undergoing Peritoneal DialysisHemantPas encore d'évaluation
- Rahman Institute of Nursing and Paramedical Sciences, Radhanagar, Guwahati Demonstration ON Peritoneal DialysisDocument7 pagesRahman Institute of Nursing and Paramedical Sciences, Radhanagar, Guwahati Demonstration ON Peritoneal DialysisPuy Puy ChhangtePas encore d'évaluation
- Interventions: Review: Anatomy and Physiology of The GU System Urine FormationDocument77 pagesInterventions: Review: Anatomy and Physiology of The GU System Urine FormationsimplyrosalynPas encore d'évaluation
- ParacentesisDocument13 pagesParacentesisroger100% (2)
- ParacenthesisDocument5 pagesParacenthesisFatimah AlshareefPas encore d'évaluation
- Procedure On Abdominal ParacentsisDocument22 pagesProcedure On Abdominal ParacentsisBhawna JoshiPas encore d'évaluation
- HemodialysisDocument2 pagesHemodialysisJanelle MarceraPas encore d'évaluation
- Abd. ParacentesisDocument45 pagesAbd. ParacentesisJosephine George JojoPas encore d'évaluation
- Foreign Body EBook MxncykDocument8 pagesForeign Body EBook MxncykErhan ErtuçPas encore d'évaluation
- Chest Drain - Evidence Based Nursing PolicyDocument7 pagesChest Drain - Evidence Based Nursing PolicyismuPas encore d'évaluation
- Peritoneal DialysisDocument31 pagesPeritoneal DialysisDani ursPas encore d'évaluation
- X Aga AaaaaaaDocument7 pagesX Aga AaaaaaaDuco Qabe WellmanPas encore d'évaluation
- Paracentesis 040641Document10 pagesParacentesis 040641Mike Faustino SolangonPas encore d'évaluation
- Nasogastric Tube InsertionDocument11 pagesNasogastric Tube InsertionDiane Kate Tobias Magno100% (1)
- I. Purpose: Clinical Practice Policy: Effective DateDocument7 pagesI. Purpose: Clinical Practice Policy: Effective DatesalamredPas encore d'évaluation
- Peritoneal DialysisDocument13 pagesPeritoneal DialysisDebasree sahaPas encore d'évaluation
- Abdominalparacentesis 131005010712 Phpapp02Document33 pagesAbdominalparacentesis 131005010712 Phpapp02Shrish Pratap SinghPas encore d'évaluation
- Ensayo Dialisis Peritoneal Erika MayoDocument17 pagesEnsayo Dialisis Peritoneal Erika Mayoerika mayoPas encore d'évaluation
- Abdominal ParacentesisDocument6 pagesAbdominal ParacentesisKhurram NadeemPas encore d'évaluation
- Inversion Utery - A Cse ReportDocument27 pagesInversion Utery - A Cse ReportJaromeKosmanPas encore d'évaluation
- Clinical Guidelines (Nursing) - Indwelling Urinary Catheter - Insertion and Ongoing CareDocument8 pagesClinical Guidelines (Nursing) - Indwelling Urinary Catheter - Insertion and Ongoing CareLeePas encore d'évaluation
- DIALYSISDocument30 pagesDIALYSISHecel Olita75% (4)
- Bladder Irrigation 4Document23 pagesBladder Irrigation 4Jay Shree100% (2)
- Assignment Dia NoDocument4 pagesAssignment Dia NoKaren T. CeletariaPas encore d'évaluation
- Paracentesis: by A.B.Sani KKB Son KTDocument8 pagesParacentesis: by A.B.Sani KKB Son KTabdulPas encore d'évaluation
- Continuous Bladder IrrigationDocument4 pagesContinuous Bladder IrrigationToto Ryan100% (2)
- The Case.Document7 pagesThe Case.Jeg B. Israel Jr.Pas encore d'évaluation
- UVC NewbornDocument6 pagesUVC NewbornMani VachaganPas encore d'évaluation
- Intravenous TherapyDocument20 pagesIntravenous TherapyFaith Tabangay ManalangPas encore d'évaluation
- HemodialysisDocument2 pagesHemodialysisEdRobertArnad100% (1)
- Paracentesis and Acites FluidDocument12 pagesParacentesis and Acites FluidNungki ArdilaPas encore d'évaluation
- Intake and Output MeasurementDocument6 pagesIntake and Output MeasurementWen RodsaPas encore d'évaluation
- IccDocument11 pagesIccranihajriPas encore d'évaluation
- Abdominal Paracentesis - Procedures - 5MinuteConsultDocument6 pagesAbdominal Paracentesis - Procedures - 5MinuteConsultJose MtzPas encore d'évaluation
- CYSTOCLYSIS3Document9 pagesCYSTOCLYSIS3Alvin OccianoPas encore d'évaluation
- Abdominal ParacentesisDocument4 pagesAbdominal ParacentesisRashmi C S100% (1)
- MCN Quiz LabDocument4 pagesMCN Quiz Labsusannah OojaPas encore d'évaluation
- Neonatal Exchange TransfusionDocument33 pagesNeonatal Exchange TransfusionedrinsnePas encore d'évaluation
- Topic: Intravenous Cannulation, Therapy and Blood TransfusionDocument32 pagesTopic: Intravenous Cannulation, Therapy and Blood TransfusionAngelica Kaye BuanPas encore d'évaluation
- Hemodialysis FinalDocument40 pagesHemodialysis Finalrose FolwersPas encore d'évaluation
- DIALYSISDocument7 pagesDIALYSISIvy E. LantapePas encore d'évaluation
- Blood Transfusion - Hatem AlsrourDocument18 pagesBlood Transfusion - Hatem Alsrourhatem alsrour100% (2)
- Thoracic and Neck TraumaDocument13 pagesThoracic and Neck Traumahatem alsrourPas encore d'évaluation
- Musculoskeletal TraumaDocument12 pagesMusculoskeletal Traumahatem alsrour100% (1)
- Triage in Emergency DepartmentDocument25 pagesTriage in Emergency Departmenthatem alsrour91% (11)
- Bipolar DisorderDocument19 pagesBipolar Disorderhatem alsrourPas encore d'évaluation
- Abdominal TraumaDocument8 pagesAbdominal Traumahatem alsrour100% (2)
- Positive & Negative Symptoms of SchizophreniaDocument1 pagePositive & Negative Symptoms of Schizophreniahatem alsrourPas encore d'évaluation
- The Cast and SplintsDocument18 pagesThe Cast and Splintshatem alsrour100% (2)
- Ventricular Arrhythmia - Hatem AlsrourDocument31 pagesVentricular Arrhythmia - Hatem Alsrourhatem alsrour100% (3)
- Crash Cart - Cardioversion & Defebrilation - Hatem AlsrourDocument17 pagesCrash Cart - Cardioversion & Defebrilation - Hatem Alsrourhatem alsrour100% (2)
- Bites & StingsDocument13 pagesBites & Stingshatem alsrour100% (2)
- Sexually Transmitted DiseasesDocument13 pagesSexually Transmitted Diseaseshatem alsrour100% (2)
- Common Drugs Used in The EmergencyDocument5 pagesCommon Drugs Used in The Emergencyhatem alsrour88% (25)
- Common Emergency DrugsDocument58 pagesCommon Emergency Drugshatem alsrour84% (19)
- Needle Cricothyroidotomy 2 - Hatem AlsrourDocument32 pagesNeedle Cricothyroidotomy 2 - Hatem Alsrourhatem alsrour100% (2)
- Burns & EscharotomyDocument36 pagesBurns & Escharotomyhatem alsrour100% (2)
- King Saud University College of NursingDocument24 pagesKing Saud University College of Nursinghatem alsrour100% (2)
- Spinal Immobilization: By: Hatem AlsrourDocument16 pagesSpinal Immobilization: By: Hatem Alsrourhatem alsrour100% (2)
- Spinal Immobilization - Hatem AlsrourDocument22 pagesSpinal Immobilization - Hatem Alsrourhatem alsrour100% (2)
- Escharotomy Incisions: Hatem AlsrourDocument28 pagesEscharotomy Incisions: Hatem Alsrourhatem alsrour100% (3)
- King Saud University College of NursingDocument49 pagesKing Saud University College of Nursinghatem alsrour100% (2)
- Needle CricothyroidotomyDocument9 pagesNeedle Cricothyroidotomyhatem alsrour100% (2)
- Blood Transfusion - Hatem AlsrourDocument18 pagesBlood Transfusion - Hatem Alsrourhatem alsrour100% (2)
- Sexually Transmitted DiseasesDocument13 pagesSexually Transmitted Diseaseshatem alsrour100% (2)
- Arrhythmia: King Saud University College of NursingDocument24 pagesArrhythmia: King Saud University College of Nursinghatem alsrour100% (2)
- King Saud University College of Nursing Gorwth & DevelopmentDocument16 pagesKing Saud University College of Nursing Gorwth & Developmenthatem alsrour100% (6)
- Crash CartDocument55 pagesCrash Carthatem alsrour100% (4)
- Vitamin Active Form Function Deficiency Disease Precursor Hypervitamin Osis SourcesDocument3 pagesVitamin Active Form Function Deficiency Disease Precursor Hypervitamin Osis Sourceshatem alsrour100% (4)
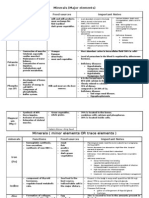
- Minerals (Major Elements) : Minera Ls Functions Food Sources Important NotesDocument3 pagesMinerals (Major Elements) : Minera Ls Functions Food Sources Important Noteshatem alsrour100% (2)
- Glyceryl Trinitrate (GTN) Infusion Chart For Chest Pain: (Or Affix Hospital Label Here)Document2 pagesGlyceryl Trinitrate (GTN) Infusion Chart For Chest Pain: (Or Affix Hospital Label Here)wasim100% (1)
- LESSON PLAN ON Hyper Emesis GravidarumDocument12 pagesLESSON PLAN ON Hyper Emesis GravidarumMadhavi ModaPas encore d'évaluation
- Search For CoursesDocument51 pagesSearch For CoursesVanessa MendezPas encore d'évaluation
- Radiometer - Blood Gas Analyzer - Abl80 Flex Operator Manual-3 (287-344)Document58 pagesRadiometer - Blood Gas Analyzer - Abl80 Flex Operator Manual-3 (287-344)Miguel FigueroaPas encore d'évaluation
- What Is An Intravenous Fluid?Document11 pagesWhat Is An Intravenous Fluid?Hayashi Breads MaaPas encore d'évaluation
- PCU Medication ListDocument11 pagesPCU Medication ListreneecolemanPas encore d'évaluation
- Treatment of Optic Neuritis With Erythropoietin (TONE) : A Randomised, Double-Blind, Placebo-Controlled Trial - Study ProtocolDocument10 pagesTreatment of Optic Neuritis With Erythropoietin (TONE) : A Randomised, Double-Blind, Placebo-Controlled Trial - Study ProtocolDyah Farah DetaPas encore d'évaluation
- Hypertensive EmergencyDocument17 pagesHypertensive EmergencyNhã PhạmPas encore d'évaluation
- Sim Scenario 4Document31 pagesSim Scenario 4lilchibaby3161Pas encore d'évaluation
- Colorectal CA With Type 2 Diabetes MellitusDocument62 pagesColorectal CA With Type 2 Diabetes MellitusJoan Rae TanPas encore d'évaluation
- HenrySchein RadiologyCatalogDocument24 pagesHenrySchein RadiologyCatalogblated1Pas encore d'évaluation
- A. Setting Up B. Inserting IV Utilizing The Dummy Arm C. Changing An IV Solution D. Discontinuing An IV InfusionDocument7 pagesA. Setting Up B. Inserting IV Utilizing The Dummy Arm C. Changing An IV Solution D. Discontinuing An IV InfusionJerika Shane MañosoPas encore d'évaluation
- 2022 Anesth s1t3 Venous Access and Fluid ManagementDocument6 pages2022 Anesth s1t3 Venous Access and Fluid ManagementMac Vince HipolitoPas encore d'évaluation
- Fisiologi Dan Kebutuhan Nutrisi PDocument277 pagesFisiologi Dan Kebutuhan Nutrisi PHeri GunawanPas encore d'évaluation
- Drugs Used in ObstetricsDocument6 pagesDrugs Used in ObstetricsJubin RajuPas encore d'évaluation
- Co AmoxiclavDocument7 pagesCo Amoxiclavbum817Pas encore d'évaluation
- Cardinal Alaris-GW - Service ManualDocument81 pagesCardinal Alaris-GW - Service ManualassistenciaPas encore d'évaluation
- R GCVP V2 2.15Document3 pagesR GCVP V2 2.15GabrielPas encore d'évaluation
- 6.pediatric SedationDocument26 pages6.pediatric SedationDirektor MilPas encore d'évaluation
- Surgical Intern Survival GuideDocument85 pagesSurgical Intern Survival Guidesgod34100% (1)
- Law FinalDocument4 pagesLaw FinalMaria Janina MarianoPas encore d'évaluation
- Answers, Rationales, and Test Taking Strategies: Managing Care Quality and SafetyDocument16 pagesAnswers, Rationales, and Test Taking Strategies: Managing Care Quality and SafetyNursyNursePas encore d'évaluation
- Ivf InsertionDocument10 pagesIvf Insertionbrilliant dumayPas encore d'évaluation
- Rotation Plan For Ward DutyDocument9 pagesRotation Plan For Ward DutyMarj Herrera0% (1)
- Drip Bag Monitoring SystemDocument58 pagesDrip Bag Monitoring SystemMuhammad Simjee100% (7)
- Medication Calculation Practice QuestionsDocument4 pagesMedication Calculation Practice QuestionsLuis RiveraPas encore d'évaluation
- Rle Case Study - Septic ShockDocument2 pagesRle Case Study - Septic Shockhazel sergioPas encore d'évaluation
- Neonatal Guidelines NHS 2011-2013Document389 pagesNeonatal Guidelines NHS 2011-2013Zuhair Aldajani زهير عمر الدجانيPas encore d'évaluation
- Dextrose Water InjectionDocument7 pagesDextrose Water InjectionNurul MazniPas encore d'évaluation
- Stihler Astotherm AP200-260 Blood Warmer - Service ManualDocument51 pagesStihler Astotherm AP200-260 Blood Warmer - Service ManualFábio Vitor MartinsPas encore d'évaluation