Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Jameswaslaski Pelvicstabilization Uploadable VersionDocument12 pagesJameswaslaski Pelvicstabilization Uploadable VersionMarco PMTPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- CapsicumDocument32 pagesCapsicumpk_shahanaPas encore d'évaluation
- Admission FormDocument4 pagesAdmission FormbharatkumarpadhiPas encore d'évaluation
- A Sample Hospital Business Plan Template - ProfitableVentureDocument15 pagesA Sample Hospital Business Plan Template - ProfitableVentureMacmilan Trevor Jamu100% (1)
- Info - Iec 62305-2 2010Document10 pagesInfo - Iec 62305-2 2010Anonymous HMhAx1BoWPas encore d'évaluation
- BBB Month 10 Workout LogDocument8 pagesBBB Month 10 Workout LogLi SaPas encore d'évaluation
- Fu Zhen and TurtleDocument7 pagesFu Zhen and Turtledrakpo100% (2)
- Grief & Loss - pptx-1Document66 pagesGrief & Loss - pptx-1pinkyPas encore d'évaluation
- Efek Klonidin Sebagai Ajuvan Anestesi Spinal Terhadap Kadar Glukose DarahDocument6 pagesEfek Klonidin Sebagai Ajuvan Anestesi Spinal Terhadap Kadar Glukose DarahRismeiniarPas encore d'évaluation
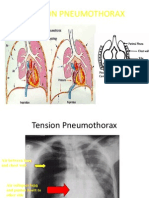
- Mer Tension PneumothoraxDocument4 pagesMer Tension PneumothoraxRismeiniarPas encore d'évaluation
- PrefaceDocument2 pagesPrefaceRismeiniarPas encore d'évaluation
- BodyDocument6 pagesBodyRismeiniarPas encore d'évaluation
- Britannia Industry LTD in India: Eat Healthy Think BetterDocument12 pagesBritannia Industry LTD in India: Eat Healthy Think BetterMayank ParasharPas encore d'évaluation
- Mandela 2017Document48 pagesMandela 2017Kibrom HaftuPas encore d'évaluation
- Worksheet 15 For Prep A: FR - ZMR.18 / R.02 / R.T: 22.09.2012 1 / 4Document4 pagesWorksheet 15 For Prep A: FR - ZMR.18 / R.02 / R.T: 22.09.2012 1 / 4elif demirelPas encore d'évaluation
- Injuries Diseases & Disorders of The Muscular SystemDocument22 pagesInjuries Diseases & Disorders of The Muscular SystemAngeli LozanoPas encore d'évaluation
- American Architecture Began With Frank Lloyd WrightDocument8 pagesAmerican Architecture Began With Frank Lloyd WrightAdheith South NgalamPas encore d'évaluation
- Bài tập tiếng anhDocument8 pagesBài tập tiếng anhLinh KhánhPas encore d'évaluation
- Kamya Life Style OpportunityDocument14 pagesKamya Life Style OpportunityMunniPas encore d'évaluation
- A Case Study of Wastewater Reclamation and Reuse in Hebei Province in China: Feasibility Analysis and Advanced Treatment DiscussionDocument2 pagesA Case Study of Wastewater Reclamation and Reuse in Hebei Province in China: Feasibility Analysis and Advanced Treatment DiscussionShalynn XiePas encore d'évaluation
- Patient Care Management Human Anatomy With Answer KeyDocument7 pagesPatient Care Management Human Anatomy With Answer KeyMarylyn Grass RootPas encore d'évaluation
- Diseases in Asian Aquaculture VIIDocument405 pagesDiseases in Asian Aquaculture VIIBurhan YusufPas encore d'évaluation
- Brad Lundmark Hired As Sun City Festival's Community ManagerDocument8 pagesBrad Lundmark Hired As Sun City Festival's Community Managerlannett40Pas encore d'évaluation
- Useful BooksDocument3 pagesUseful BooksphuongfeoPas encore d'évaluation
- Sodium Metabisulfite SDSDocument8 pagesSodium Metabisulfite SDSChaib AhmedPas encore d'évaluation
- GuidelinesDocument7 pagesGuidelinesAnariza TahaPas encore d'évaluation
- Chapter 1Document6 pagesChapter 1Abegail Joy AragonPas encore d'évaluation
- Amber Sewell: Professional SummaryDocument4 pagesAmber Sewell: Professional Summaryapi-383979726Pas encore d'évaluation
- CCC Breast Feeding PolicyDocument1 pageCCC Breast Feeding PolicyVictorPas encore d'évaluation
- Gout Guide: Lifelong Transformation, One Healthy Habit at A Time®Document9 pagesGout Guide: Lifelong Transformation, One Healthy Habit at A Time®Rocco McWhitebeardPas encore d'évaluation
- Kangaroo Mother Care Rooming in UpdatedDocument44 pagesKangaroo Mother Care Rooming in UpdatedStar DustPas encore d'évaluation
- Abnormal Lie: - Abnormal Lie Consists of Two Types: Transverse Lie Oblique LieDocument21 pagesAbnormal Lie: - Abnormal Lie Consists of Two Types: Transverse Lie Oblique LieBharat ThapaPas encore d'évaluation
- Topic 13Document23 pagesTopic 13hasvinPas encore d'évaluation
- BHS InggrisDocument4 pagesBHS InggrisarifinilhamPas encore d'évaluation