Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
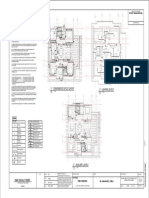
- Electrical Layout and SchedulesDocument2 pagesElectrical Layout and Schedulesberolyan0688% (8)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Revised National Plumbing Code of The PhilippinesDocument225 pagesRevised National Plumbing Code of The Philippinesberolyan0694% (16)
- Vaccination Records - AdultsDocument2 pagesVaccination Records - AdultsverumluxPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Basic Plumbing SymbolsDocument1 pageBasic Plumbing SymbolsBrandon Borromeo75% (4)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- CSI DivisionDocument5 pagesCSI Divisionberolyan06Pas encore d'évaluation
- Implant Failure and ManagementDocument59 pagesImplant Failure and ManagementDrIbrahimShaikh0% (1)
- The New National Building CodeDocument16 pagesThe New National Building Codegeanndyngenlyn86% (50)
- Comparative Analysis of PD 957 & BP 220Document4 pagesComparative Analysis of PD 957 & BP 220berolyan0690% (10)
- Loading Dock System GuideDocument38 pagesLoading Dock System Guideberolyan06Pas encore d'évaluation
- Loading Dock System GuideDocument38 pagesLoading Dock System Guideberolyan06Pas encore d'évaluation
- Auditorium Acoustics 101: The Quieter, the BetterDocument8 pagesAuditorium Acoustics 101: The Quieter, the BetterCharles NukesevenPas encore d'évaluation
- Intestinal Obstruction 4Document25 pagesIntestinal Obstruction 4Muvenn KannanPas encore d'évaluation
- Cognitive DisabilitiesDocument4 pagesCognitive Disabilitieshannalee13Pas encore d'évaluation
- 2a. Atspph ScaleDocument2 pages2a. Atspph Scaleyani0707Pas encore d'évaluation
- Filipino ArchitectsDocument2 pagesFilipino ArchitectsKevin SolanoyPas encore d'évaluation
- Review Article: Guided Bone Regeneration: A Literature ReviewDocument16 pagesReview Article: Guided Bone Regeneration: A Literature ReviewGonçalo Gomes SanchesPas encore d'évaluation
- Revised IRR BP220 2008Document75 pagesRevised IRR BP220 2008anyerieramranle100% (5)
- Online ExamsDocument14 pagesOnline Examsberolyan06Pas encore d'évaluation
- Structural ReviewerDocument18 pagesStructural ReviewerJay EmPas encore d'évaluation
- UtilitiesDocument8 pagesUtilitiesberolyan06Pas encore d'évaluation
- PlanningDocument3 pagesPlanningberolyan06Pas encore d'évaluation
- Csi Division ArchitecturalDocument6 pagesCsi Division Architecturalberolyan06100% (1)
- Structural ReviewerDocument5 pagesStructural Reviewerberolyan06Pas encore d'évaluation
- Archl ReviewerDocument89 pagesArchl Reviewerberolyan06Pas encore d'évaluation
- Famous Dictums/Philosophies/Sayings: "Form Follows Function"Document2 pagesFamous Dictums/Philosophies/Sayings: "Form Follows Function"Rachelle JacosalemPas encore d'évaluation
- Architectural Technologies: MaterialsDocument14 pagesArchitectural Technologies: Materialsberolyan06Pas encore d'évaluation
- Active Review Center: History of ArchitectureDocument7 pagesActive Review Center: History of Architectureberolyan06Pas encore d'évaluation
- Forensic ExamDocument46 pagesForensic Examberolyan06Pas encore d'évaluation
- TechnologyDocument35 pagesTechnologyberolyan06Pas encore d'évaluation
- Berol SPDocument25 pagesBerol SPberolyan06Pas encore d'évaluation
- ConceptsDocument25 pagesConceptsberolyan06Pas encore d'évaluation
- Forensic AnalysisDocument12 pagesForensic Analysisberolyan06Pas encore d'évaluation
- ORAL PRECURSOR LESION DIAGNOSIS AND MANAGEMENTDocument51 pagesORAL PRECURSOR LESION DIAGNOSIS AND MANAGEMENTberolyan06Pas encore d'évaluation
- Milwaukee Public MarketDocument27 pagesMilwaukee Public Marketberolyan06100% (1)
- IRRPD957Document66 pagesIRRPD957berolyan06Pas encore d'évaluation
- Career Map - DoctorDocument7 pagesCareer Map - DoctorAdityaPas encore d'évaluation
- Study DesignDocument130 pagesStudy Designephremtigabie7Pas encore d'évaluation
- Studies On The Stability of Chicken IgY in Different Sugars Complex Carbohydrates and Food MaterialsDocument12 pagesStudies On The Stability of Chicken IgY in Different Sugars Complex Carbohydrates and Food MaterialsJohnrel SecretariaPas encore d'évaluation
- Seizures in The Preterm NeonateDocument10 pagesSeizures in The Preterm NeonateRoosevelt Santibañez Dla TorrePas encore d'évaluation
- Team Code 34 RDocument23 pagesTeam Code 34 RShivam TiwaryPas encore d'évaluation
- Unconventional Fixed Partial Denture: A Simple Solution For Aesthetic RehabilitationDocument4 pagesUnconventional Fixed Partial Denture: A Simple Solution For Aesthetic RehabilitationAdvanced Research PublicationsPas encore d'évaluation
- The Use of Contraceptives in Nigeria: Benefits, Challenges and Probable SolutionsDocument13 pagesThe Use of Contraceptives in Nigeria: Benefits, Challenges and Probable SolutionsShaguolo O. JosephPas encore d'évaluation
- HC09 ErgonomicsDocument29 pagesHC09 ErgonomicsRegina LiePas encore d'évaluation
- The Stuart Stress Adaptation Model of Psychiatric Nursing CareDocument3 pagesThe Stuart Stress Adaptation Model of Psychiatric Nursing CareScott PuckettPas encore d'évaluation
- Efficacy and Safety of Rabeprazole in Children.20Document10 pagesEfficacy and Safety of Rabeprazole in Children.20Ismy HoiriyahPas encore d'évaluation
- Slavin 1996Document6 pagesSlavin 1996jahdsdjad asffdhsajhajdkPas encore d'évaluation
- Hernia Repair Surgery ExplainedDocument13 pagesHernia Repair Surgery Explainedbugoy_bugoyPas encore d'évaluation
- TranslateeDocument6 pagesTranslateeAmalia Tri UtamiPas encore d'évaluation
- MD AANOADocument21 pagesMD AANOARizka Dany AfinaPas encore d'évaluation
- Unit 4: Medical EmergenciesDocument44 pagesUnit 4: Medical EmergenciesMR々๛ AKMツPas encore d'évaluation
- Respiratory Procedures: Tracheal Intubation PreparationDocument46 pagesRespiratory Procedures: Tracheal Intubation PreparationRhea Andrea UyPas encore d'évaluation
- Cover Letter To The EditorDocument2 pagesCover Letter To The EditorMohamed GhaliPas encore d'évaluation
- Basic ImmunologyDocument2 pagesBasic ImmunologyadibwanPas encore d'évaluation
- Pharmacology Lab (1) : Routes of Drug AdministrationDocument14 pagesPharmacology Lab (1) : Routes of Drug AdministrationBotan AbdullahPas encore d'évaluation
- Instructions For Use: Home Sperm Test For Male FertilityDocument2 pagesInstructions For Use: Home Sperm Test For Male FertilityRAVAN ZJPas encore d'évaluation
- For The Best Sinus Congestion RemediesDocument4 pagesFor The Best Sinus Congestion Remedies4zaleakuPas encore d'évaluation
- Chapter 026 CoagulationDocument7 pagesChapter 026 Coagulationthubtendrolma100% (3)
- Vaccine Research StatusDocument112 pagesVaccine Research StatusJunko Tsukuda100% (1)
- Common Teratogens and Their EffectsDocument3 pagesCommon Teratogens and Their EffectsThyataira chuaPas encore d'évaluation