Vous aimerez peut-être aussi
- Peck and Peck JCDocument38 pagesPeck and Peck JCdoctorneha66100% (1)
- Labial BowDocument70 pagesLabial Bowdoctorneha6660% (5)
- SpringsDocument33 pagesSpringsdoctorneha66100% (1)
- Labial BowsDocument39 pagesLabial Bowsdoctorneha6660% (5)
- The Airway and Facial Development Collaborative: Episode 13 Dr. Keith ThorntonDocument8 pagesThe Airway and Facial Development Collaborative: Episode 13 Dr. Keith Thorntondoctorneha66Pas encore d'évaluation
- MetrologyDocument10 pagesMetrologydoctorneha66Pas encore d'évaluation
- 30 April - 2 May 2011 Berjaya Times Square Hotel, Kuala LumpurDocument2 pages30 April - 2 May 2011 Berjaya Times Square Hotel, Kuala Lumpurdoctorneha66Pas encore d'évaluation
- Tweed CorrectionDocument5 pagesTweed Correctiondoctorneha66Pas encore d'évaluation
- Abbreviations Used in PrescrptionsDocument14 pagesAbbreviations Used in Prescrptionsdoctorneha66Pas encore d'évaluation
- Cardiac Glycosides & Drug Herapy of Heart FailureDocument113 pagesCardiac Glycosides & Drug Herapy of Heart Failuredoctorneha66Pas encore d'évaluation
- Fundamental Operations in Compunding, PPTDocument32 pagesFundamental Operations in Compunding, PPTdoctorneha6691% (22)
- Drug Treatment of AnemiaDocument36 pagesDrug Treatment of Anemiadoctorneha66Pas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Sesi 6-Fisiologi Neuromuskuler IDocument86 pagesSesi 6-Fisiologi Neuromuskuler IGisellePas encore d'évaluation
- La Cirrhose Alcoolique: Aspects Épidémiologiques, Diagnostiques Et ÉvolutifsDocument3 pagesLa Cirrhose Alcoolique: Aspects Épidémiologiques, Diagnostiques Et ÉvolutifsLoic MCPas encore d'évaluation
- Definingacutekidney Injury: Siddharth Verma,, John A. KellumDocument16 pagesDefiningacutekidney Injury: Siddharth Verma,, John A. KellumNicolas Peña RiveraPas encore d'évaluation
- Git MotilityDocument68 pagesGit MotilityGaurav SinghPas encore d'évaluation
- Daftar Pustaka FXDocument3 pagesDaftar Pustaka FXstroma januariPas encore d'évaluation
- Respiratory Quiz: Student Academic Learning ServicesDocument4 pagesRespiratory Quiz: Student Academic Learning ServicesFREDRICKPas encore d'évaluation
- Utmb Absite Review ManualDocument245 pagesUtmb Absite Review ManualEl Gonzo100% (1)
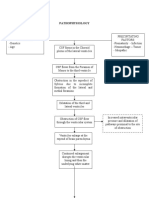
- Hydrocephalus PathophysiologyDocument3 pagesHydrocephalus PathophysiologyErika CadawanPas encore d'évaluation
- Dialysis Treatment - A Comprehensive DescriptionDocument13 pagesDialysis Treatment - A Comprehensive Descriptionrmprskgwk5Pas encore d'évaluation
- Summary of Nervous SystemDocument4 pagesSummary of Nervous SystemDerel PatriaPas encore d'évaluation
- Body Tissues: 17. The Four Major Tissue Types Are Named in Figure 3-9. For Each TissueDocument9 pagesBody Tissues: 17. The Four Major Tissue Types Are Named in Figure 3-9. For Each TissueSireRyūjinSkylerPas encore d'évaluation
- Obstetric and Newborn Care IDocument184 pagesObstetric and Newborn Care ISabrina SarpongPas encore d'évaluation
- Anatomy and Physiology of The Goat PDFDocument7 pagesAnatomy and Physiology of The Goat PDFHannan MirzaPas encore d'évaluation
- PHD ThesisDocument166 pagesPHD Thesisandreea_vornicu25Pas encore d'évaluation
- Anatomy and Physiology Science Olympiad 2024 Cheat SheetDocument3 pagesAnatomy and Physiology Science Olympiad 2024 Cheat Sheetgfzmrtqj54Pas encore d'évaluation
- DIET in Chronic Kidney DiseaseDocument3 pagesDIET in Chronic Kidney Diseaseatul_desai_3Pas encore d'évaluation
- ANATOMY and PHYSIOLOGY of CHRONIC OTITIS MEDIA-GCS Sa MED - ANNEX-maam ValezaDocument36 pagesANATOMY and PHYSIOLOGY of CHRONIC OTITIS MEDIA-GCS Sa MED - ANNEX-maam ValezaBonieve Pitogo NoblezadaPas encore d'évaluation
- Chapter 16: Autonomic Nervous System: Multiple ChoiceDocument15 pagesChapter 16: Autonomic Nervous System: Multiple ChoiceGolf2153Pas encore d'évaluation
- Urinary Tract Infection Anatomy and PhysiologyDocument12 pagesUrinary Tract Infection Anatomy and PhysiologyPaul Anthony Centeno PimentelPas encore d'évaluation
- Nerves and Reflexes: 1 of 14 © Boardworks LTD 2011Document14 pagesNerves and Reflexes: 1 of 14 © Boardworks LTD 2011A.K MonPas encore d'évaluation
- Sulaiman, Akbar, Lesmana Dan Noer. 2007. Buku Ajar Ilmu Penyakit Hati. Jakarta: JayabadiDocument2 pagesSulaiman, Akbar, Lesmana Dan Noer. 2007. Buku Ajar Ilmu Penyakit Hati. Jakarta: JayabadiNenden Kartika DeviPas encore d'évaluation
- Hepatobiliary DiseaseDocument60 pagesHepatobiliary DiseaseFirdaus AslamPas encore d'évaluation
- Respiratory SystemDocument23 pagesRespiratory Systemjimboy baddiriPas encore d'évaluation
- Male Genitalia Clinical - Physical Examination - Mark H. SwartzDocument3 pagesMale Genitalia Clinical - Physical Examination - Mark H. Swartzmaha candraPas encore d'évaluation
- Chapter 15 - Hormones & Endocrine GlandsDocument17 pagesChapter 15 - Hormones & Endocrine Glandsapi-3728508100% (1)
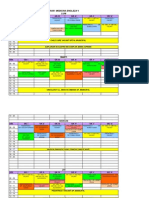
- Orar Medicina Engleza V Luni: ORA Gr. I Gr. Ii Gr. Iii Gr. Iv Gr. V Gr. ViDocument3 pagesOrar Medicina Engleza V Luni: ORA Gr. I Gr. Ii Gr. Iii Gr. Iv Gr. V Gr. ViCornel MihaiPas encore d'évaluation
- The Importance of Endocrine GlandsDocument4 pagesThe Importance of Endocrine GlandsMark Vincent Lacbain SaguinPas encore d'évaluation
- Management of Heart Failure With Preserved EjectionFraction A Review PDFDocument13 pagesManagement of Heart Failure With Preserved EjectionFraction A Review PDFGharbi StrongPas encore d'évaluation
- Fundamentals of Urine & Body Fluid Analysis 5th Edition 2023 ALGRAWANYDocument461 pagesFundamentals of Urine & Body Fluid Analysis 5th Edition 2023 ALGRAWANYDr-Issam IrakPas encore d'évaluation
- Small and Large Intestines-0Document23 pagesSmall and Large Intestines-0Siraj ShiferawPas encore d'évaluation