Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Max GrowthDocument63 pagesMax GrowthRoney Jennifer Abraham100% (1)
- The A-Z Medical WritingDocument153 pagesThe A-Z Medical WritingNikhil Mali100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Destroying Fat ThibaudeuDocument31 pagesDestroying Fat ThibaudeuOrlando Paez Cortazar100% (1)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Hiv in PregnancyDocument29 pagesHiv in PregnancyIrfan FauziPas encore d'évaluation
- Hiv in PregnancyDocument29 pagesHiv in PregnancyIrfan FauziPas encore d'évaluation
- NUTRITION GUIDE T-Monster New Plan PDFDocument17 pagesNUTRITION GUIDE T-Monster New Plan PDFAnthony Dinicolantonio0% (1)
- Self Heal Holistic ApproachDocument9 pagesSelf Heal Holistic ApproachShebin Sam Sajan100% (1)
- Green Smoothie RecipesDocument12 pagesGreen Smoothie RecipesAngelaPas encore d'évaluation
- Efficacy of Cognitive Behaviour Therapy in ManagementDocument5 pagesEfficacy of Cognitive Behaviour Therapy in ManagementIrfan FauziPas encore d'évaluation
- Stop COVID (19) Cold - Dr. Mercola 2020Document17 pagesStop COVID (19) Cold - Dr. Mercola 2020petr18Pas encore d'évaluation
- Lesson Plan On PemDocument19 pagesLesson Plan On Pemanil jain0% (1)
- Hamilton Anxiety Rating Scale (HAM-A)Document2 pagesHamilton Anxiety Rating Scale (HAM-A)Elsa Ameliana ManurungPas encore d'évaluation
- Guidelines ASPENDocument138 pagesGuidelines ASPENJaqueline Odair100% (1)
- First-Time Fathers ' Experiences of Parenting During The First YearDocument12 pagesFirst-Time Fathers ' Experiences of Parenting During The First YearIrfan FauziPas encore d'évaluation
- Daily Action Plan of A ChampionDocument2 pagesDaily Action Plan of A ChampionIrfan FauziPas encore d'évaluation
- Boet Tiger 2017Document12 pagesBoet Tiger 2017Irfan FauziPas encore d'évaluation
- OsteoporosisDocument23 pagesOsteoporosisIrfan FauziPas encore d'évaluation
- Growth Chart CDC PDFDocument203 pagesGrowth Chart CDC PDFIrfan FauziPas encore d'évaluation
- Peran PPNI Utk Perawat Global INGGRISDocument17 pagesPeran PPNI Utk Perawat Global INGGRISIrfan FauziPas encore d'évaluation
- Growth Chart CDC PDFDocument203 pagesGrowth Chart CDC PDFIrfan FauziPas encore d'évaluation
- Blank Daily Action Planner PDFDocument1 pageBlank Daily Action Planner PDFIrfan FauziPas encore d'évaluation
- (8th) HospitalizationDocument18 pages(8th) HospitalizationIrfan FauziPas encore d'évaluation
- Substannce Related DisorderDocument16 pagesSubstannce Related DisorderIrfan FauziPas encore d'évaluation
- Daily Action Plan of A ChampionDocument2 pagesDaily Action Plan of A ChampionIrfan FauziPas encore d'évaluation
- NIH Public AccessDocument17 pagesNIH Public AccessIrfan FauziPas encore d'évaluation
- Far Milo 2014Document1 pageFar Milo 2014Irfan FauziPas encore d'évaluation
- Analisa Gas DarahDocument8 pagesAnalisa Gas DarahIrfan FauziPas encore d'évaluation
- The Cardiac Children's Hospital Early Warning Score (C-CHEWS)Document8 pagesThe Cardiac Children's Hospital Early Warning Score (C-CHEWS)Irfan FauziPas encore d'évaluation
- Cho 2016Document9 pagesCho 2016Irfan FauziPas encore d'évaluation
- Efficacy of Cognitive-Behavioral TherapyDocument20 pagesEfficacy of Cognitive-Behavioral TherapyIrfan FauziPas encore d'évaluation
- Pa Shik Anti 2012Document8 pagesPa Shik Anti 2012Irfan FauziPas encore d'évaluation
- Barton 2003Document7 pagesBarton 2003Irfan FauziPas encore d'évaluation
- Comparison of The Effects of Yoga and LSM-1Document5 pagesComparison of The Effects of Yoga and LSM-1Irfan FauziPas encore d'évaluation
- Physical Abuse Around The Time of PregnancyDocument6 pagesPhysical Abuse Around The Time of PregnancyIrfan FauziPas encore d'évaluation
- Diabetic Education and Management Report and ToolDocument89 pagesDiabetic Education and Management Report and ToolIrfan FauziPas encore d'évaluation
- The "Reading The Mind in The Eyes" Test Revised Version - A Study With Normal Adults, and Adults With Asperger Syndrome or High-Functioning Autis PDFDocument11 pagesThe "Reading The Mind in The Eyes" Test Revised Version - A Study With Normal Adults, and Adults With Asperger Syndrome or High-Functioning Autis PDFIrfan FauziPas encore d'évaluation
- DSM5Update2015 PDFDocument30 pagesDSM5Update2015 PDFIrfan FauziPas encore d'évaluation
- KemotherapiDocument8 pagesKemotherapiIrfan FauziPas encore d'évaluation
- International Dairy Journal: Sebastian Chalupa-Krebzdak, Chloe J. Long, Benjamin M. BohrerDocument9 pagesInternational Dairy Journal: Sebastian Chalupa-Krebzdak, Chloe J. Long, Benjamin M. BohrerNikolett NagyPas encore d'évaluation
- Avian Urolithiasis EngDocument4 pagesAvian Urolithiasis Engwaseem234Pas encore d'évaluation
- Should Government Impose Restrictions On What Kinds of Foods Can Be Served in School CafeteriasDocument9 pagesShould Government Impose Restrictions On What Kinds of Foods Can Be Served in School CafeteriasharonPas encore d'évaluation
- List of Indonesian Canned Fish Exporters: Indonesian Trade Promotion Center (Itpc - Osaka)Document2 pagesList of Indonesian Canned Fish Exporters: Indonesian Trade Promotion Center (Itpc - Osaka)SudarismanPas encore d'évaluation
- Meal Planning Part 1Document38 pagesMeal Planning Part 1Nirvana SuggiePas encore d'évaluation
- MCQ - Online - 1500 QuestionsDocument262 pagesMCQ - Online - 1500 QuestionsNfPas encore d'évaluation
- Catering Menu For INSET 2023Document3 pagesCatering Menu For INSET 2023jenisaPas encore d'évaluation
- Form "D-1" Annual Return (See 2020-2021 General Information: Regulation 2.1.13)Document2 pagesForm "D-1" Annual Return (See 2020-2021 General Information: Regulation 2.1.13)Shiv KumarPas encore d'évaluation
- Congresbrochure EngDocument48 pagesCongresbrochure EngPedro BrugadaPas encore d'évaluation
- Diet Chart For Glowing Skin Patient, Diet For Glowing Skin Chart LybrateDocument1 pageDiet Chart For Glowing Skin Patient, Diet For Glowing Skin Chart Lybrateshy91Pas encore d'évaluation
- DBR Notes EssayDocument4 pagesDBR Notes EssayLisa -Pas encore d'évaluation
- Chemistry Project Class XIIDocument11 pagesChemistry Project Class XIIPherands Pherands0% (1)
- Iq 1Document5 pagesIq 1Endrianus Jaya PutraPas encore d'évaluation
- Assessing Cereal Quality ParametersDocument5 pagesAssessing Cereal Quality ParametersMilling and Grain magazinePas encore d'évaluation
- Eating A Balanced DietDocument3 pagesEating A Balanced DietmarinahuamaniPas encore d'évaluation
- Author Guidelines - IfTDocument14 pagesAuthor Guidelines - IfTmahe_sce4702Pas encore d'évaluation
- Chapathi With Underutilized Seeds and Food WasteDocument70 pagesChapathi With Underutilized Seeds and Food WasteRuby JayaseelanPas encore d'évaluation
- Pre Workout - Citrulline - Malaat - Citrulline - Malate - Poeder300g - v2-90220MLDocument1 pagePre Workout - Citrulline - Malaat - Citrulline - Malate - Poeder300g - v2-90220MLDebbaghPas encore d'évaluation
- KarbohidratDocument55 pagesKarbohidratAhmad FirmanPas encore d'évaluation
- 6 Day Cutting Routine For Weight Loss PDFDocument5 pages6 Day Cutting Routine For Weight Loss PDF.,j bPas encore d'évaluation
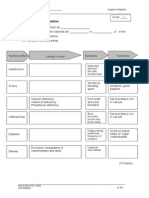
- WORKSHEET 6.3 MalnutritionDocument4 pagesWORKSHEET 6.3 MalnutritionLim Wai Wai SmktpPas encore d'évaluation
- A Stepwise Enteral Nutrition Algorithm For Critically (Susan Dan Nilesh Mehta)Document7 pagesA Stepwise Enteral Nutrition Algorithm For Critically (Susan Dan Nilesh Mehta)NyomanGinaHennyKristiantiPas encore d'évaluation