Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Ilga Worldmap 2015 EngDocument2 pagesIlga Worldmap 2015 EngarieasmitaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Home Emergency Book PDFDocument260 pagesHome Emergency Book PDFrahulmultivision100% (1)
- Drug Doses 2017Document127 pagesDrug Doses 2017Yuliawati HarunaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Home Emergency Book PDFDocument260 pagesHome Emergency Book PDFrahulmultivision100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Cuidados Diabetes 2016Document119 pagesCuidados Diabetes 2016Diego Pizarro ReyesPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- JNC8 HTNDocument2 pagesJNC8 HTNTaradifaNurInsi0% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- PRINAN DrowningDocument7 pagesPRINAN DrowningarieasmitaPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
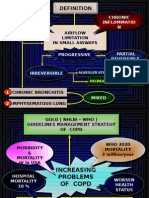
- Copd New InsightDocument31 pagesCopd New InsightarieasmitaPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Guidelines Recommendations Newborn HealthDocument17 pagesGuidelines Recommendations Newborn HealtharieasmitaPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Bathing of The Healthy NewbornDocument2 pagesBathing of The Healthy NewbornarieasmitaPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- (S N) W4.5 - Must Read - Post-Partum Care WHO 2013.pdf Http://bsquochoai - Ga - BsquochoaiDocument72 pages(S N) W4.5 - Must Read - Post-Partum Care WHO 2013.pdf Http://bsquochoai - Ga - Bsquochoaidrquochoai100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Acls 2000Document12 pagesAcls 2000arieasmitaPas encore d'évaluation
- Nenny Anggraeni PDFDocument21 pagesNenny Anggraeni PDFarieasmitaPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Gambaran Radiologi Efusi Pleura Dan Pneumothorax: Dr. Hj. Nurwita A, SP - Rad, MhkesDocument1 pageGambaran Radiologi Efusi Pleura Dan Pneumothorax: Dr. Hj. Nurwita A, SP - Rad, MhkesGumam M. Bintang RamandaPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- New Microsoft Office Word 97 - 2003 DocumentDocument1 pageNew Microsoft Office Word 97 - 2003 DocumentarieasmitaPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Chamanismo Colonialismo y El Hombre Salvaje Michael TaussigDocument1 pageChamanismo Colonialismo y El Hombre Salvaje Michael TaussigAndrésSotoPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Thoracic Trauma: EMS Professions Temple CollegeDocument96 pagesThoracic Trauma: EMS Professions Temple CollegearieasmitaPas encore d'évaluation
- Simian Foamy Viruses (SFV)Document21 pagesSimian Foamy Viruses (SFV)arieasmitaPas encore d'évaluation
- Akses Vena Central: Anestesiologi Dan Reanimasi RSUD TasikmalayaDocument28 pagesAkses Vena Central: Anestesiologi Dan Reanimasi RSUD TasikmalayaSaeful AmbariPas encore d'évaluation
- The Cardiovascular System: The Heart: Human Anatomy & Physiology, Sixth EditionDocument37 pagesThe Cardiovascular System: The Heart: Human Anatomy & Physiology, Sixth EditionJeramie DeanPas encore d'évaluation
- EMT Basic Scenario - Cardiovascular Emergencies - Scenario 1Document2 pagesEMT Basic Scenario - Cardiovascular Emergencies - Scenario 1Jaypz Del100% (1)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Pre-Hospital Assessment Sheet: Triage ScoreDocument2 pagesPre-Hospital Assessment Sheet: Triage Scoreratna purwitasariPas encore d'évaluation
- Biology Investigatory ProjectDocument61 pagesBiology Investigatory ProjectJIYA NAIR66% (61)
- This Study Resource Was: ScenarioDocument8 pagesThis Study Resource Was: ScenarioabychloePas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Cardiovascular ActivitiesDocument8 pagesCardiovascular ActivitiesJuan RuizPas encore d'évaluation
- BplogDocument2 pagesBplogMonir AhamedPas encore d'évaluation
- Checklist Cardiac AssessmentDocument8 pagesChecklist Cardiac AssessmentLovely GopezPas encore d'évaluation
- NEWBORN ASSESSMENT DajuuuuuuuuuuuuuuuuDocument31 pagesNEWBORN ASSESSMENT Dajuuuuuuuuuuuuuuuuamal abdulrahmanPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- AUTOPSY ReezuDocument16 pagesAUTOPSY ReezuBnB UsmlePas encore d'évaluation
- Thrombolysis For Acute Myocardial Infarction: Clinical Cardiology: New FrontiersDocument15 pagesThrombolysis For Acute Myocardial Infarction: Clinical Cardiology: New FrontiersBinod KumarPas encore d'évaluation
- Kinesiotaping LinfedemaDocument2 pagesKinesiotaping LinfedemaLuis Miguel AlferezPas encore d'évaluation
- BIOPSYCHOLOGYDocument25 pagesBIOPSYCHOLOGYLizzie ShodiyaPas encore d'évaluation
- ReflexesDocument7 pagesReflexesShaine Dominique SantosPas encore d'évaluation
- ArobicDocument4 pagesArobicrishitPas encore d'évaluation
- Everest/First Ascents: Altitude Danger Begins in PhericheDocument2 pagesEverest/First Ascents: Altitude Danger Begins in PhericheIrigoyen APas encore d'évaluation
- Clinical Case ScenarioDocument3 pagesClinical Case ScenarioHolly CividinPas encore d'évaluation
- Case Study-HomeostasisDocument2 pagesCase Study-HomeostasisAllaika Zyrah FloresPas encore d'évaluation
- Drug Study: (Sodium Bicarbonate)Document5 pagesDrug Study: (Sodium Bicarbonate)dodovs0% (1)
- Acute Respiratory FailureDocument5 pagesAcute Respiratory FailureHoney Bee S. PlatolonPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Burns An Introduction To Burns and Basic Wound - 2023 - Physician Assistant CliDocument11 pagesBurns An Introduction To Burns and Basic Wound - 2023 - Physician Assistant CliJose AnaconaPas encore d'évaluation
- Physio Blood TransDocument7 pagesPhysio Blood TransRoderick PalattaoPas encore d'évaluation
- Human Body System InfographicDocument12 pagesHuman Body System InfographicDiana VillanuevaPas encore d'évaluation
- Artigos Científicos - NeCDocument905 pagesArtigos Científicos - NeCBryan JulioPas encore d'évaluation
- Definition - Mecical Term - KEYDocument4 pagesDefinition - Mecical Term - KEYKieu AnhPas encore d'évaluation
- Chapter 10 Respiratory System PresentationDocument48 pagesChapter 10 Respiratory System PresentationMary Jane LubricoPas encore d'évaluation
- hORmones in Plants Class Note Class 10 ...Document4 pageshORmones in Plants Class Note Class 10 ...AceHunterPas encore d'évaluation
- 2017 - Howe - Advanced Resistance Training Strategies For Increasing Muscle Hypertrophy and Maximal StrengthDocument7 pages2017 - Howe - Advanced Resistance Training Strategies For Increasing Muscle Hypertrophy and Maximal StrengthJuanPas encore d'évaluation
- AmlodipineDocument9 pagesAmlodipineMA 09Pas encore d'évaluation
- Acute Pain ManagementDocument31 pagesAcute Pain ManagementTherese Jane TiradorPas encore d'évaluation