Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Writing Letters of Recommendation: A Guide For USC-SOM Greenville FacultyDocument7 pagesWriting Letters of Recommendation: A Guide For USC-SOM Greenville FacultyUmaPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Sample Strong Eras Lor 5-05Document1 pageSample Strong Eras Lor 5-05Raiyan KhanPas encore d'évaluation
- Types of AnemiaDocument11 pagesTypes of AnemiaCHRISTIE MONTANO50% (2)
- ASHP Injectable Drug Information A Comprehensive Guide To Compatibility and Stability-1Document1 757 pagesASHP Injectable Drug Information A Comprehensive Guide To Compatibility and Stability-1reza100% (3)
- ERAS Letter of Recommendations Guidelines Updated All 1Document5 pagesERAS Letter of Recommendations Guidelines Updated All 1ddddjjjPas encore d'évaluation
- ERAS Letter of Recommendations Guidelines Updated All 1Document5 pagesERAS Letter of Recommendations Guidelines Updated All 1ddddjjjPas encore d'évaluation
- D H ADocument250 pagesD H AKath Cuevas0% (1)
- Introduction To AnaesthesiaDocument24 pagesIntroduction To AnaesthesiaDeobrat DwivediPas encore d'évaluation
- Nail PsoriasisDocument13 pagesNail PsoriasisAira KellyPas encore d'évaluation
- Aspartame's DangersDocument67 pagesAspartame's DangersCrazy LukePas encore d'évaluation
- Nursing Audit Tool PDFDocument12 pagesNursing Audit Tool PDFjamiePas encore d'évaluation
- Strong Letter RecommendationDocument2 pagesStrong Letter RecommendationJorge Luis Sánchez Alarcón100% (1)
- Writing Letters of RecommendationDocument4 pagesWriting Letters of Recommendationwenskyrose1100% (1)
- Writing Good and Honest Recommendations - BerlacherDocument19 pagesWriting Good and Honest Recommendations - BerlacherUmaPas encore d'évaluation
- Improving The Letter of Recommendation: Jeremy D. Prager, MD, Charles M. Myer III, MD, and Myles L. Pensak, MDDocument4 pagesImproving The Letter of Recommendation: Jeremy D. Prager, MD, Charles M. Myer III, MD, and Myles L. Pensak, MDUmaPas encore d'évaluation
- Annals of Diagnostic Pathology: On The Subject of Writing Letters of RecommendationDocument2 pagesAnnals of Diagnostic Pathology: On The Subject of Writing Letters of RecommendationUmaPas encore d'évaluation
- The Utility of Letters of Recommendation in Predicting Resident Success: Can The ACGME Competencies Help?Document4 pagesThe Utility of Letters of Recommendation in Predicting Resident Success: Can The ACGME Competencies Help?UmaPas encore d'évaluation
- Professionalism: Plagiarised Letters of Recommendation Submitted For The National Resident Matching ProgramDocument9 pagesProfessionalism: Plagiarised Letters of Recommendation Submitted For The National Resident Matching ProgramUmaPas encore d'évaluation
- AAIM Perspectives: A B C D e F G H I JDocument6 pagesAAIM Perspectives: A B C D e F G H I JUmaPas encore d'évaluation
- Perception of Female Buttocks and Breast PDFDocument8 pagesPerception of Female Buttocks and Breast PDFJuan Manuel Caycho CervantesPas encore d'évaluation
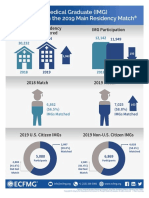
- Match 2019 Info GraphicDocument1 pageMatch 2019 Info GraphicUmaPas encore d'évaluation
- Gas, Bloating, and Belching: Approach To Evaluation and ManagementDocument11 pagesGas, Bloating, and Belching: Approach To Evaluation and ManagementUmaPas encore d'évaluation
- Gas, Bloating, and Belching: Approach To Evaluation and ManagementDocument11 pagesGas, Bloating, and Belching: Approach To Evaluation and ManagementUmaPas encore d'évaluation
- New Text DocupastestmentDocument3 pagesNew Text DocupastestmentUmaPas encore d'évaluation
- CPG ObesityDocument34 pagesCPG ObesityΑθηνάPas encore d'évaluation
- UW PharmacologyDocument1 pageUW PharmacologyUmaPas encore d'évaluation
- 3 EngDocument126 pages3 EngUmaPas encore d'évaluation
- New Text DocumentDocument11 pagesNew Text DocumentUmaPas encore d'évaluation
- New Text DocudsfsdfmentDocument34 pagesNew Text DocudsfsdfmentUmaPas encore d'évaluation
- Medicine Primary Care OrthopaedicsDocument1 pageMedicine Primary Care OrthopaedicsUmaPas encore d'évaluation
- UW PharmacologyDocument1 pageUW PharmacologyUmaPas encore d'évaluation
- Eathe.2016.1080p.webrip.x264.aac2.0 StuttershitDocument38 pagesEathe.2016.1080p.webrip.x264.aac2.0 StuttershitUmaPas encore d'évaluation
- JuDocument3 pagesJuUmaPas encore d'évaluation
- I Didn't Know That:: Worse at NightDocument2 pagesI Didn't Know That:: Worse at NightUmaPas encore d'évaluation
- PEDocument1 pagePEUmaPas encore d'évaluation
- Https WWW - Ghc.org All-Sites Guidelines Heart-FailureDocument23 pagesHttps WWW - Ghc.org All-Sites Guidelines Heart-FailureUmaPas encore d'évaluation
- KeyDocument1 pageKeyUmaPas encore d'évaluation
- UntitledDocument12 pagesUntitledjhony192Pas encore d'évaluation
- Ingles Tarea 1Document3 pagesIngles Tarea 1Daniela Carolina LaraPas encore d'évaluation
- BSc Medical Sociology Syllabus DetailsDocument24 pagesBSc Medical Sociology Syllabus Detailsmchakra72100% (2)
- Government Initiatives in Health and Nutrition: Vinod PaulDocument29 pagesGovernment Initiatives in Health and Nutrition: Vinod PaulMani KandanPas encore d'évaluation
- Exercise DepressionDocument17 pagesExercise Depressionlakshminivas PingaliPas encore d'évaluation
- Activity 2 Finals Histo Lab - EDLAY2ADocument2 pagesActivity 2 Finals Histo Lab - EDLAY2ATom Anthony TonguiaPas encore d'évaluation
- Introduction of Cancer Center in KMUHDocument36 pagesIntroduction of Cancer Center in KMUHSantoPas encore d'évaluation
- Identifying ErrorsDocument2 pagesIdentifying ErrorsLourdes Marianne MenesesPas encore d'évaluation
- A Sociofugal Space for Privacy in ConsultationDocument7 pagesA Sociofugal Space for Privacy in ConsultationDennis Villaruz-AliasPas encore d'évaluation
- Amlodipine Side EffectsDocument6 pagesAmlodipine Side Effects1976gt500Pas encore d'évaluation
- Guidelines For Treatment of Infections in Primary Care in Hull and East RidingDocument22 pagesGuidelines For Treatment of Infections in Primary Care in Hull and East RidingSiLvia Riska PratiwiPas encore d'évaluation
- Cefuroxime Drug StudyDocument1 pageCefuroxime Drug StudyDUMANGENG ELLAINE D.Pas encore d'évaluation
- Endophthalmitis 1Document42 pagesEndophthalmitis 1Nasrin sultana rmcPas encore d'évaluation
- Patient Safety Practices and Medical Errors: Perception of Health Care Providers at Jimma University Specialized Hospital, Southwest EthiopiaDocument9 pagesPatient Safety Practices and Medical Errors: Perception of Health Care Providers at Jimma University Specialized Hospital, Southwest Ethiopiamahadabrata21Pas encore d'évaluation
- Radical NephrectomyDocument3 pagesRadical NephrectomyBiggs JuntillaPas encore d'évaluation
- NU 120 Skin Integrity - Care - PlanDocument4 pagesNU 120 Skin Integrity - Care - Planmrsfelic08100% (3)
- Nurses' Postoperative Pain Management PracticesDocument6 pagesNurses' Postoperative Pain Management PracticesIndah PratiwiPas encore d'évaluation
- List of Books Box # 35: S.No. Author Title Year Edition Vol Call #Document10 pagesList of Books Box # 35: S.No. Author Title Year Edition Vol Call #lubs123Pas encore d'évaluation
- DAFTAR PUSTAKADocument2 pagesDAFTAR PUSTAKAChristopher GarrettPas encore d'évaluation
- Delfinm QsenDocument57 pagesDelfinm Qsenapi-346220114Pas encore d'évaluation
- Pulmonary Embolism: Presented By: Miss. M.K.Kaku Nursing TutorDocument9 pagesPulmonary Embolism: Presented By: Miss. M.K.Kaku Nursing TutorKaku ManishaPas encore d'évaluation
- Jisakos 2017 000146 PDFDocument10 pagesJisakos 2017 000146 PDFemilPas encore d'évaluation
- Bananasap FinalDocument20 pagesBananasap FinalKarina Lingan100% (1)