Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Unit Vi. Polymeric Materials: Topic OutlineDocument7 pagesUnit Vi. Polymeric Materials: Topic OutlineIvyy Joyce BuanPas encore d'évaluation
- Interior FinishesDocument45 pagesInterior FinishesBradley TaylorPas encore d'évaluation
- Protein Bioplastic - AlvinDocument5 pagesProtein Bioplastic - AlvinLevine98Pas encore d'évaluation
- 1 Thermo and Equil - Remedial - AnswerDocument6 pages1 Thermo and Equil - Remedial - AnswerNur Afiqah Mohd ZakiPas encore d'évaluation
- English-Arristan 66Document3 pagesEnglish-Arristan 66asebaei95Pas encore d'évaluation
- (Plastics Design Library) Carlos Federico Jasso-Gastinel, José M. Kenny - Modification of Polymer Properties-William Andrew (2017)Document222 pages(Plastics Design Library) Carlos Federico Jasso-Gastinel, José M. Kenny - Modification of Polymer Properties-William Andrew (2017)Monique BarretoPas encore d'évaluation
- Filament Winding and PultrusionDocument14 pagesFilament Winding and PultrusionEsha AkhterPas encore d'évaluation
- Catalog DatronDocument136 pagesCatalog DatrongeorgegvrPas encore d'évaluation
- CH4 - Jan 2014Document15 pagesCH4 - Jan 2014Kieran RichardsPas encore d'évaluation
- High Density Polyethylene ReportDocument2 pagesHigh Density Polyethylene ReportHamzah A. LaftaPas encore d'évaluation
- Air CellDocument3 pagesAir CellSathish Kumar APas encore d'évaluation
- What Is PU Leather? All-In-One Overview of Latest PU Leather !!Document7 pagesWhat Is PU Leather? All-In-One Overview of Latest PU Leather !!nurseerror9Pas encore d'évaluation
- Biomaterials-Introduction: Bio Material - It Is ADocument33 pagesBiomaterials-Introduction: Bio Material - It Is APoornimaPas encore d'évaluation
- Tablet FriabilityDocument25 pagesTablet FriabilityJean Florencondia67% (3)
- Flexographic Ink Formulations and Structures AppendixDocument58 pagesFlexographic Ink Formulations and Structures AppendixMilos Papic100% (2)
- Colour and Art A Brief History of PigmentDocument9 pagesColour and Art A Brief History of PigmentHua Hidari YangPas encore d'évaluation
- Curlsbot's List of Curly Girl IngredientsDocument3 pagesCurlsbot's List of Curly Girl Ingredientsraphaela_zadielPas encore d'évaluation
- 04 - Organic SynthesisDocument45 pages04 - Organic SynthesisMerrene Bright Divino JudanPas encore d'évaluation
- UV-Curing Coatings: A Concise OverviewDocument10 pagesUV-Curing Coatings: A Concise OverviewIsmail BayraktarPas encore d'évaluation
- MasterBook 1 Eng PDFDocument64 pagesMasterBook 1 Eng PDFDaniel CîrsteaPas encore d'évaluation
- Strength & Properties of Modal Rayon FibreDocument16 pagesStrength & Properties of Modal Rayon FibreSohaib Anas100% (1)
- Transparent Specialties INEOSDocument42 pagesTransparent Specialties INEOSInês MorgadoPas encore d'évaluation
- Progress in Used Tyres Management in The European Union: A ReviewDocument12 pagesProgress in Used Tyres Management in The European Union: A ReviewAnonymous lPFeDds1gAPas encore d'évaluation
- Scope of Maxillofacial Prosthesis Materials: From Past To Future-A Literature ReviewDocument4 pagesScope of Maxillofacial Prosthesis Materials: From Past To Future-A Literature ReviewNishanthini AnnamalaiPas encore d'évaluation
- Carbohydrates: Classification, Structures and FunctionsDocument35 pagesCarbohydrates: Classification, Structures and FunctionsSunita SharmaPas encore d'évaluation
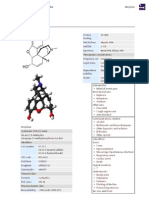
- MorphineDocument13 pagesMorphineAli Sayed100% (2)
- Caswick SS404Document1 pageCaswick SS404Anorld WalkerPas encore d'évaluation
- Esd Wristbands: Comfortable and Anti-AllergenicDocument9 pagesEsd Wristbands: Comfortable and Anti-AllergenicNicolas Pastine SepulvedaPas encore d'évaluation
- Pembuatan Dan Karakterisasi Komposit SerDocument5 pagesPembuatan Dan Karakterisasi Komposit Serhadi sufyanPas encore d'évaluation
- Acid Resistant Rubber Lining & Liquid CoatingsDocument81 pagesAcid Resistant Rubber Lining & Liquid CoatingsSikander AleemPas encore d'évaluation