Vous aimerez peut-être aussi
- Disseminated Intravacular Coagulation (DIC) 2Document12 pagesDisseminated Intravacular Coagulation (DIC) 2Radya AgnaPas encore d'évaluation
- Ireland in Pre Celtic TimesDocument398 pagesIreland in Pre Celtic TimesGrant MacDonald100% (5)
- Aircraft ChecksDocument10 pagesAircraft ChecksAshirbad RathaPas encore d'évaluation
- Reaction rate determination and simulation of hydrogenation processDocument3 pagesReaction rate determination and simulation of hydrogenation processToMemPas encore d'évaluation
- Interpretasi Urine RutinDocument118 pagesInterpretasi Urine Rutinboy jendri huluPas encore d'évaluation
- TiroidDocument26 pagesTiroidJoni Riana MustaqimPas encore d'évaluation
- Acute Myocardial InfarctionDocument32 pagesAcute Myocardial InfarctionListya Normalita100% (1)
- IEC-60721-3-3-2019 (Enviromental Conditions)Document12 pagesIEC-60721-3-3-2019 (Enviromental Conditions)Electrical DistributionPas encore d'évaluation
- Trauma BuliDocument32 pagesTrauma BulimoonlightsoantaPas encore d'évaluation
- Oracle Fusion Financials Book Set Home Page SummaryDocument274 pagesOracle Fusion Financials Book Set Home Page SummaryAbhishek Agrawal100% (1)
- Hemoroid Interna Laporan KasusDocument4 pagesHemoroid Interna Laporan KasusSarah Humaira DennisonPas encore d'évaluation
- Shock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentDocument64 pagesShock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentHarika BandaruPas encore d'évaluation
- What Is Rack Chock SystemDocument7 pagesWhat Is Rack Chock SystemSarah Perez100% (1)
- Hipertensi-Krisis Dr. HendroDocument35 pagesHipertensi-Krisis Dr. Hendroyudhagp100% (1)
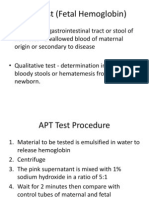
- APT Test (Fetal Hemoglobin)Document11 pagesAPT Test (Fetal Hemoglobin)Diovic TanPas encore d'évaluation
- Twin To Twin Transfusion PDFDocument26 pagesTwin To Twin Transfusion PDFAmbreen Z MalikPas encore d'évaluation
- Chronic Liver DiseaseDocument3 pagesChronic Liver DiseaseMohammad AbbasPas encore d'évaluation
- GI Diseases Lecture on IBSDocument9 pagesGI Diseases Lecture on IBSEmeraldyModyPas encore d'évaluation
- Using Snapchat For OSINT - Save Videos Without OverlaysDocument12 pagesUsing Snapchat For OSINT - Save Videos Without OverlaysVo TinhPas encore d'évaluation
- Pancreatic MalignancyDocument22 pagesPancreatic Malignancylovelots1234Pas encore d'évaluation
- Icd XDocument3 pagesIcd XR Ghianesya GantinaPas encore d'évaluation
- (INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Document10 pages(INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Yolanda FitrianiPas encore d'évaluation
- Ortho Fraktur 1/3 Proximal Humerus DextraDocument57 pagesOrtho Fraktur 1/3 Proximal Humerus DextraFian ChristoPas encore d'évaluation
- OsteomielitisDocument28 pagesOsteomielitismaulidaangraini100% (1)
- LAPORAN PORTOFOLIO PROGRAM INTERNSIPDocument43 pagesLAPORAN PORTOFOLIO PROGRAM INTERNSIPEndang Susilowati NPas encore d'évaluation
- 17 Brain VascularizationDocument86 pages17 Brain VascularizationMuhammad RidwanPas encore d'évaluation
- DRUG ERUPTION GUIDEDocument46 pagesDRUG ERUPTION GUIDESyahDikaPas encore d'évaluation
- Management of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientDocument12 pagesManagement of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientRani Dwi NPas encore d'évaluation
- Sindrom NefrotikDocument22 pagesSindrom NefrotikGyta Apriati100% (1)
- Diagnosis Dan Diagnosis Banding DM SK 2Document99 pagesDiagnosis Dan Diagnosis Banding DM SK 2syahron maskatPas encore d'évaluation
- 5.soap Chest PainDocument19 pages5.soap Chest PainDesiana Kemala SariPas encore d'évaluation
- KARDIOMYOPATI: Understanding Heart Muscle DiseasesDocument28 pagesKARDIOMYOPATI: Understanding Heart Muscle DiseasesArif Zulfian MubarokPas encore d'évaluation
- Diabetes Mellitus Pada Anak KuliahDocument51 pagesDiabetes Mellitus Pada Anak KuliahNisha AnggiaPas encore d'évaluation
- Drug Eruption Fix PrintDocument30 pagesDrug Eruption Fix PrintAshari MohpulPas encore d'évaluation
- K4. Diagnosis Holistik - EngDocument21 pagesK4. Diagnosis Holistik - EngBevila KorspoilvilPas encore d'évaluation
- Basic Life Support (BLS) Support (Acls) : Dan Advance Cardiac LifeDocument27 pagesBasic Life Support (BLS) Support (Acls) : Dan Advance Cardiac LifeRuth AngeliaPas encore d'évaluation
- IPDIDocument30 pagesIPDIaris budionoPas encore d'évaluation
- Palmoplantar PustulosisDocument3 pagesPalmoplantar PustulosisRobby ZayendraPas encore d'évaluation
- Final Assignment of Big Data in Hospital Wendry Pasorong MHM Batch 3 UphDocument11 pagesFinal Assignment of Big Data in Hospital Wendry Pasorong MHM Batch 3 UphwendryPas encore d'évaluation
- Referat Buerger DiseaseDocument19 pagesReferat Buerger DiseaseSyahmi SyafiqPas encore d'évaluation
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- A Clinical Study of Etiology and Management of Acute Intestinal ObstructionDocument6 pagesA Clinical Study of Etiology and Management of Acute Intestinal ObstructionFalon PapalangiPas encore d'évaluation
- Materi To Interna 02 FebruariDocument75 pagesMateri To Interna 02 FebruariMario AlexanderPas encore d'évaluation
- Kul Sem 4 Heat Stroke N Fever UHT 2016Document63 pagesKul Sem 4 Heat Stroke N Fever UHT 2016NandaSuryaWijayaPas encore d'évaluation
- K23 - Text Book Reading MiopatiDocument28 pagesK23 - Text Book Reading MiopatiNaila SyifaPas encore d'évaluation
- Jurnal Reading Rome IVDocument31 pagesJurnal Reading Rome IVrizki febrianPas encore d'évaluation
- CASE REPORT 4: PNEUMONIA DEXTRA SUSPECT COVID-19 + ACUTE GASTRITISDocument17 pagesCASE REPORT 4: PNEUMONIA DEXTRA SUSPECT COVID-19 + ACUTE GASTRITISdianarahimmPas encore d'évaluation
- Congenital Adrenal HyperplasiaDocument2 pagesCongenital Adrenal HyperplasiaesyPas encore d'évaluation
- Sindrom Nefritik DebDocument2 pagesSindrom Nefritik DebrchristevenPas encore d'évaluation
- DIABETES MELITUS TYPE 2 MANAGEMENT UNDER 35 YEAR OLD WOMANDocument10 pagesDIABETES MELITUS TYPE 2 MANAGEMENT UNDER 35 YEAR OLD WOMANMeta SakinaPas encore d'évaluation
- Refreshing DHFDocument13 pagesRefreshing DHFNia Nurhayati ZakiahPas encore d'évaluation
- Lapkas Fournier GangreneDocument29 pagesLapkas Fournier GangreneDavid Rainer Irianto HutajuluPas encore d'évaluation
- Alopecia AreataDocument13 pagesAlopecia AreataAchoonk RamadhanPas encore d'évaluation
- Ulkus PeptikumDocument30 pagesUlkus PeptikumRizky Indah SorayaPas encore d'évaluation
- Diabetes Mellitus: DR Hiew Fu LiongDocument30 pagesDiabetes Mellitus: DR Hiew Fu LiongamminsaffriPas encore d'évaluation
- Diabetic Foot Ulcer ClassificationDocument17 pagesDiabetic Foot Ulcer ClassificationAriski Pratama JohanPas encore d'évaluation
- Diabetes Melitus: Dr. Ihsanil Husna, SPPDDocument67 pagesDiabetes Melitus: Dr. Ihsanil Husna, SPPDnathan timothyPas encore d'évaluation
- LAPORAN TUTORIAL SKENARIO C BLOK 22 THALASSEMIADocument47 pagesLAPORAN TUTORIAL SKENARIO C BLOK 22 THALASSEMIAAnusha PrakashPas encore d'évaluation
- HHS - Resistensi InsulinDocument22 pagesHHS - Resistensi InsulinKristina Puspa DewiPas encore d'évaluation
- Diabetic Foot: by Myrna Rita PMRDocument33 pagesDiabetic Foot: by Myrna Rita PMRDianNurlitaAnggrainiPas encore d'évaluation
- Understanding Acute Leukemia and ThalassemiaDocument39 pagesUnderstanding Acute Leukemia and ThalassemialeilaPas encore d'évaluation
- Journal Reading THT - OMADocument15 pagesJournal Reading THT - OMAIndira MaycellaPas encore d'évaluation
- Diabetes Melitus & PengelolaannyaDocument56 pagesDiabetes Melitus & PengelolaannyaIbnuPas encore d'évaluation
- Diagnosing Chest Pain and Shortness of BreathDocument2 pagesDiagnosing Chest Pain and Shortness of BreathIndah SariPas encore d'évaluation
- Managing Acute Metabolic Complications of Diabetes: HHS TreatmentDocument24 pagesManaging Acute Metabolic Complications of Diabetes: HHS TreatmentAnnisaPas encore d'évaluation
- Systemic Lupus Erythematosus: Pathogenesis and Clinical FeaturesDocument30 pagesSystemic Lupus Erythematosus: Pathogenesis and Clinical FeaturesOrion JohnPas encore d'évaluation
- Summary of Medical EmergenciesDocument24 pagesSummary of Medical Emergenciesbasharswork99Pas encore d'évaluation
- Adrenal Glands MS2Document38 pagesAdrenal Glands MS2Tatiana Leashe WootenPas encore d'évaluation
- Telecare Collaborative Management of Chronic Pain in Primary 222Document13 pagesTelecare Collaborative Management of Chronic Pain in Primary 222Listya NormalitaPas encore d'évaluation
- Dermatitis Herpetiformis: Timo L. Reunala, MDDocument9 pagesDermatitis Herpetiformis: Timo L. Reunala, MDListya NormalitaPas encore d'évaluation
- The Cardiac CircleDocument75 pagesThe Cardiac CircleListya NormalitaPas encore d'évaluation
- Glaucoma American Journal of OphtalmologyDocument7 pagesGlaucoma American Journal of OphtalmologyListya NormalitaPas encore d'évaluation
- 3 LOed-bedah Islam 33 - 41Document13 pages3 LOed-bedah Islam 33 - 41Listya NormalitaPas encore d'évaluation
- Contact Dermatitis BJD Guidelines May 2009Document9 pagesContact Dermatitis BJD Guidelines May 2009Cynthia OktariszaPas encore d'évaluation
- 2009 Stovamesis blok 24 Skills Lab BLS Neurologis cedera kepala Spinal Aspek forensikDocument1 page2009 Stovamesis blok 24 Skills Lab BLS Neurologis cedera kepala Spinal Aspek forensikListya NormalitaPas encore d'évaluation
- Scabies Diagnosis and ManagementDocument5 pagesScabies Diagnosis and ManagementAbdul Rauf ZakariaPas encore d'évaluation
- Fisiologi Batuk: Mekanisme Refleks dan Reseptor BatukDocument25 pagesFisiologi Batuk: Mekanisme Refleks dan Reseptor BatukListya NormalitaPas encore d'évaluation
- Fisiologi Batuk: Mekanisme Refleks dan Reseptor BatukDocument25 pagesFisiologi Batuk: Mekanisme Refleks dan Reseptor BatukListya NormalitaPas encore d'évaluation
- Change Angle of Optic Nerve and Ocular Orbit With Age BJO PDFDocument6 pagesChange Angle of Optic Nerve and Ocular Orbit With Age BJO PDFListya NormalitaPas encore d'évaluation
- FURUNCULOSISDocument4 pagesFURUNCULOSISListya NormalitaPas encore d'évaluation
- 24th Block-Trauma & Emergencies: Kegawatan Gastrointestinal Kegawatdaruratan ObsginDocument2 pages24th Block-Trauma & Emergencies: Kegawatan Gastrointestinal Kegawatdaruratan ObsginListya NormalitaPas encore d'évaluation
- Manajemen Trauma Tumpul AbdomenDocument10 pagesManajemen Trauma Tumpul AbdomenListya NormalitaPas encore d'évaluation
- Analisis Data Low Back PainDocument9 pagesAnalisis Data Low Back PainListya NormalitaPas encore d'évaluation
- Evaluasi Dan Indikasi LaparotomyDocument6 pagesEvaluasi Dan Indikasi LaparotomyListya NormalitaPas encore d'évaluation
- REP ML2 FertilityDocument13 pagesREP ML2 FertilityListya NormalitaPas encore d'évaluation
- Splenic Injury GuidelineDocument3 pagesSplenic Injury GuidelineListya NormalitaPas encore d'évaluation
- Partus Lama SBG Indikasi Emergensi SCDocument9 pagesPartus Lama SBG Indikasi Emergensi SCListya NormalitaPas encore d'évaluation
- Enteral Vs Parenteral Nutrition After Major Abdominal SurgeryDocument0 pageEnteral Vs Parenteral Nutrition After Major Abdominal SurgeryListya NormalitaPas encore d'évaluation
- Abnormal Labor-ModifiedDocument8 pagesAbnormal Labor-ModifiedListya NormalitaPas encore d'évaluation
- Sushilseminarctev 121219014859 Phpapp01Document93 pagesSushilseminarctev 121219014859 Phpapp01Listya NormalitaPas encore d'évaluation
- Rheumatoid ArtritisDocument56 pagesRheumatoid ArtritisListya NormalitaPas encore d'évaluation
- Blunt Splenic TraumaDocument6 pagesBlunt Splenic TraumaListya NormalitaPas encore d'évaluation
- Airway & Breathing Manaj DR BambangDocument50 pagesAirway & Breathing Manaj DR BambangListya NormalitaPas encore d'évaluation
- Blunt Abdominal TraumaDocument0 pageBlunt Abdominal TraumaListya NormalitaPas encore d'évaluation
- Intec Waste PresiDocument8 pagesIntec Waste Presiapi-369931794Pas encore d'évaluation
- The Invisible Hero Final TNDocument8 pagesThe Invisible Hero Final TNKatherine ShenPas encore d'évaluation
- Presentation On Ich Topics & Guidelines With A Special Reference ToDocument79 pagesPresentation On Ich Topics & Guidelines With A Special Reference ToVidyaPas encore d'évaluation
- Accidental PoisoningDocument3 pagesAccidental PoisoningBRUELIN MELSHIA MPas encore d'évaluation
- SQL 1: Basic Statements: Yufei TaoDocument24 pagesSQL 1: Basic Statements: Yufei TaoHui Ka HoPas encore d'évaluation
- Practical LPM-122Document31 pagesPractical LPM-122anon_251667476Pas encore d'évaluation
- BỘ GIÁO DỤC VÀ ĐÀO TẠO ĐỀ THI HỌC PHẦN KINH TẾ VĨ MÔDocument5 pagesBỘ GIÁO DỤC VÀ ĐÀO TẠO ĐỀ THI HỌC PHẦN KINH TẾ VĨ MÔPhạm Thu NgaPas encore d'évaluation
- A.2.3. Passive Transport Systems MCQsDocument3 pagesA.2.3. Passive Transport Systems MCQsPalanisamy SelvamaniPas encore d'évaluation
- Hardware Purchase and Sales System Project ProfileDocument43 pagesHardware Purchase and Sales System Project Profilesanjaykumarguptaa100% (2)
- Credit Risk Management Practice in Private Banks Case Study Bank of AbyssiniaDocument85 pagesCredit Risk Management Practice in Private Banks Case Study Bank of AbyssiniaamognePas encore d'évaluation
- Mark Dean GR6211 Fall 2018 Columbia University: - Choice Theory'Document5 pagesMark Dean GR6211 Fall 2018 Columbia University: - Choice Theory'bhaskkarPas encore d'évaluation
- Chapter 9-10 (PPE) Reinzo GallegoDocument48 pagesChapter 9-10 (PPE) Reinzo GallegoReinzo GallegoPas encore d'évaluation
- Ch. 7 - Audit Reports CA Study NotesDocument3 pagesCh. 7 - Audit Reports CA Study NotesUnpredictable TalentPas encore d'évaluation
- Design and Analysis of Algorithms Prof. Madhavan Mukund Chennai Mathematical Institute Week - 01 Module - 01 Lecture - 01Document8 pagesDesign and Analysis of Algorithms Prof. Madhavan Mukund Chennai Mathematical Institute Week - 01 Module - 01 Lecture - 01SwatiPas encore d'évaluation
- Introduction To Streering Gear SystemDocument1 pageIntroduction To Streering Gear SystemNorman prattPas encore d'évaluation
- Impact of Recruitment & Selection on Employee RetentionDocument39 pagesImpact of Recruitment & Selection on Employee RetentiongizawPas encore d'évaluation
- 67c Series Bulletin 08 04 PDFDocument12 pages67c Series Bulletin 08 04 PDFnight wolfPas encore d'évaluation
- Bethany Getz ResumeDocument2 pagesBethany Getz Resumeapi-256325830Pas encore d'évaluation
- Phys114 Ps 1Document11 pagesPhys114 Ps 1Reine Amabel JarudaPas encore d'évaluation
- Obsolescence 2. Book Value 3. Depreciation 4. Depletion EtcDocument9 pagesObsolescence 2. Book Value 3. Depreciation 4. Depletion EtcKHAN AQSAPas encore d'évaluation
- Manual - Sentron Pac Profibus Do Modul - 2009 02 - en PDFDocument106 pagesManual - Sentron Pac Profibus Do Modul - 2009 02 - en PDFDante Renee Mendoza DelgadoPas encore d'évaluation
- Future Design of Accessibility in Games - A Design Vocabulary - ScienceDirectDocument16 pagesFuture Design of Accessibility in Games - A Design Vocabulary - ScienceDirectsulaPas encore d'évaluation