Vous aimerez peut-être aussi
- Management of Tuberculosis: A guide for clinicians (eBook edition)D'EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Pas encore d'évaluation
- Colorectal CancerDocument7 pagesColorectal Cancerjames garciaPas encore d'évaluation
- Colorectal CancerDocument3 pagesColorectal CancerAriane May Rubio50% (2)
- Casestudy Gastric CarcinomaDocument53 pagesCasestudy Gastric CarcinomaAngelaTrinidadPas encore d'évaluation
- Liver Cancer Pathophysiology: Predisposing FactorDocument3 pagesLiver Cancer Pathophysiology: Predisposing FactorTarantado100% (2)
- Liver CancerDocument27 pagesLiver CancerKoRnflakes100% (4)
- Pathophysiology of Breast CancerDocument3 pagesPathophysiology of Breast Cancerpauline mangadaPas encore d'évaluation
- Liver CancerDocument1 pageLiver CancerTarantado67% (3)
- Pathophysiology Breast CancerDocument3 pagesPathophysiology Breast CancerNathalie kate petallarPas encore d'évaluation
- Colorectal CancerDocument14 pagesColorectal Cancershaqtim100% (2)
- Breast CancerDocument11 pagesBreast CancerRock'nRoll Buddies100% (2)
- CholelithiasisDocument5 pagesCholelithiasisrgflores1979100% (2)
- Cervical CADocument32 pagesCervical CAEvangel Padua100% (2)
- Pathophysiology of Breast CancerDocument4 pagesPathophysiology of Breast CancerChiqui Lao DumanhugPas encore d'évaluation
- Breast Cancer PathophysiologyDocument17 pagesBreast Cancer PathophysiologySwit Tapican MaangPas encore d'évaluation
- Colon Cancer Case StudyDocument18 pagesColon Cancer Case Studyapi-271062060100% (2)
- Etiology and Pathophysiology Breast CancerDocument1 pageEtiology and Pathophysiology Breast Cancermay_hisolerPas encore d'évaluation
- A Case Study On Rectal AdenocarcinomaDocument62 pagesA Case Study On Rectal AdenocarcinomaEyySiEffVee100% (1)
- Pathophysiology of Esophageal CADocument2 pagesPathophysiology of Esophageal CAroshmae100% (4)
- Colorectal CancerDocument50 pagesColorectal CancerHans Chester Rirao Capinding100% (2)
- Acute PancreatitisDocument40 pagesAcute Pancreatitisjpacheco39100% (4)
- Pathophysiology of Liver Cancer 2Document3 pagesPathophysiology of Liver Cancer 2Charis Paroginog92% (12)
- Pancreatic Cancer - PresentationDocument71 pagesPancreatic Cancer - PresentationMavy CantonPas encore d'évaluation
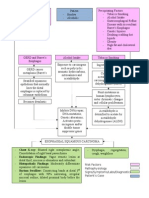
- SCHEMATIC DIAGRAM Obstructive JaundiceDocument1 pageSCHEMATIC DIAGRAM Obstructive JaundiceJan Niño EstrellaPas encore d'évaluation
- Pa Tho Physiology of Hodgkin'sDocument10 pagesPa Tho Physiology of Hodgkin'sIvica Rae100% (1)
- Ovarian New GrowthDocument7 pagesOvarian New GrowthRegiena Tamargo100% (1)
- Case Study-Breast CADocument11 pagesCase Study-Breast CAJoanna Cabildo83% (6)
- Bladder Cancer: By: Estigoy, Harriet and Galang, Cuttie AnneDocument18 pagesBladder Cancer: By: Estigoy, Harriet and Galang, Cuttie AnneCuttie Anne Galang100% (1)
- Vii. Nursing Care Plan: Secretions in The AirwaysDocument5 pagesVii. Nursing Care Plan: Secretions in The AirwaysJai - Ho100% (2)
- Breast CancerDocument33 pagesBreast Canceredenpearlcastillo67% (3)
- Lung Ca Case Presentation PDFDocument28 pagesLung Ca Case Presentation PDFapi-276417422100% (2)
- 4.2 Pathophysiology Breast CADocument1 page4.2 Pathophysiology Breast CAaeglaecakamariaPas encore d'évaluation
- Cancer of The ColonDocument8 pagesCancer of The Colonnot your medz duranPas encore d'évaluation
- Mastectomy Case StudyDocument9 pagesMastectomy Case StudyAura Regene AtienzaPas encore d'évaluation
- Gastric Cancer: Calag, Prescilla Tavas, Charme FayeDocument20 pagesGastric Cancer: Calag, Prescilla Tavas, Charme FayeDareRaymond0% (1)
- Obstructive JaundiceDocument54 pagesObstructive JaundiceJenine Ezra M. Conol50% (2)
- Uterine Cancer Pa Tho PhysiologyDocument17 pagesUterine Cancer Pa Tho PhysiologyJeneva L. Lauzon100% (2)
- Cancer Case StudyDocument23 pagesCancer Case StudyJaymica Laggui DacquilPas encore d'évaluation
- Colon CancerDocument17 pagesColon CancerYaska MusaPas encore d'évaluation
- Nursing Care in RadiotherapyDocument26 pagesNursing Care in Radiotherapyحسام جبار مجيد100% (1)
- Epidemiology, Pathogenesis, and Pathology of NeuroblastomaDocument21 pagesEpidemiology, Pathogenesis, and Pathology of NeuroblastomaHandre PutraPas encore d'évaluation
- Breast CancerDocument53 pagesBreast CancerChristine Karen Ang Suarez100% (3)
- Pathophysiology of Adenocarcinoma, Moderately DifferentiatedDocument5 pagesPathophysiology of Adenocarcinoma, Moderately Differentiatedmacel sibayan33% (3)
- AML Case StudyDocument66 pagesAML Case StudyNoel Christian PeraltaPas encore d'évaluation
- Breast Cancer Case StudyDocument5 pagesBreast Cancer Case StudyFrancesca ElixirPas encore d'évaluation
- BREAST CANCERppt NCM 106 Updated July 7Document103 pagesBREAST CANCERppt NCM 106 Updated July 7sweet25chocolat100% (1)
- Colorectal CancerDocument8 pagesColorectal Cancerjorgeacct100% (3)
- A Case Study On Renal CancerDocument30 pagesA Case Study On Renal CancerAiyish CapunoPas encore d'évaluation
- Pathophysiology of BREAST CANCERDocument1 pagePathophysiology of BREAST CANCEREggy Pascual100% (1)
- Pathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorsDocument1 pagePathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorstatiPas encore d'évaluation
- Vaginal CancerDocument11 pagesVaginal CancerAiko TokunagaPas encore d'évaluation
- Case PresentationDocument25 pagesCase PresentationElva Oktiana Rahmi80% (5)
- Breast Cancer PathophysiologyDocument2 pagesBreast Cancer PathophysiologyErba100% (7)
- JaundiceDocument29 pagesJaundiceMurali TiarasanPas encore d'évaluation
- CHOLECYSTECTOMYDocument35 pagesCHOLECYSTECTOMYfaitheee100% (3)
- Nursing Care Plan Breast-CancerDocument2 pagesNursing Care Plan Breast-CancerGreg Llandelar100% (2)
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Liver CancerDocument44 pagesLiver CancerJoyce Ann CumlatPas encore d'évaluation
- Cancer of LiverDocument14 pagesCancer of LiverRani SujithPas encore d'évaluation
- StrabismusDocument30 pagesStrabismusEjay Jacob Ricamara100% (1)
- Laryngeal CarcinomaDocument52 pagesLaryngeal CarcinomaEjay Jacob Ricamara67% (3)
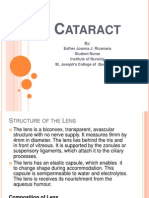
- CataractDocument53 pagesCataractEjay Jacob RicamaraPas encore d'évaluation
- Diseases of The Ear Otitis Media, Foreign Bodies in The Ears, MastoiditisDocument69 pagesDiseases of The Ear Otitis Media, Foreign Bodies in The Ears, MastoiditisEjay Jacob RicamaraPas encore d'évaluation
- Wilms TumorDocument38 pagesWilms TumorEjay Jacob RicamaraPas encore d'évaluation
- ParagonimiasisDocument3 pagesParagonimiasisEjay Jacob RicamaraPas encore d'évaluation
- Pott's Disease or Tuberculosis in The SpineDocument7 pagesPott's Disease or Tuberculosis in The SpineEjay Jacob RicamaraPas encore d'évaluation
- Drug Study - DexamethasoneDocument2 pagesDrug Study - DexamethasoneEjay Jacob RicamaraPas encore d'évaluation
- NorvascDocument1 pageNorvascEjay Jacob RicamaraPas encore d'évaluation
- LasixDocument1 pageLasixEjay Jacob RicamaraPas encore d'évaluation
- Nodular Nontoxic GoiterDocument4 pagesNodular Nontoxic GoiterEjay Jacob RicamaraPas encore d'évaluation
- Pneumothorax..final Doc. For Case PresDocument4 pagesPneumothorax..final Doc. For Case PresEjay Jacob RicamaraPas encore d'évaluation
- Infra-Auricular Mass Case PresDocument8 pagesInfra-Auricular Mass Case PresEjay Jacob RicamaraPas encore d'évaluation
- Cerebrovascular Accident Case PresDocument27 pagesCerebrovascular Accident Case PresEjay Jacob RicamaraPas encore d'évaluation
- Chronic Hepatitis BDocument5 pagesChronic Hepatitis BMurat HessesPas encore d'évaluation
- A Histopathological Study of Liver in 118 Cases of Cirrhosis 2167 0889 1000193 PDFDocument7 pagesA Histopathological Study of Liver in 118 Cases of Cirrhosis 2167 0889 1000193 PDFHemin HassanPas encore d'évaluation
- Giovanna FatovichDocument16 pagesGiovanna FatovichGilang Kurnia Hirawati0% (1)
- Drug Induced Liver Injury Secondary To Herbal and Dietary SupplementsDocument15 pagesDrug Induced Liver Injury Secondary To Herbal and Dietary Supplementsalejandro toro riveraPas encore d'évaluation
- Robert G. Gish, MD CV - January 2014Document221 pagesRobert G. Gish, MD CV - January 2014Robert G. Gish, MDPas encore d'évaluation
- Prevention of HerpatitisDocument54 pagesPrevention of Herpatitisapi-270822363Pas encore d'évaluation
- HBP MCQsDocument67 pagesHBP MCQsNessreen JamalPas encore d'évaluation
- 007-Hepatobiliary & PancreaticDocument59 pages007-Hepatobiliary & PancreaticAhmed ZaghwPas encore d'évaluation
- Liver Cancer Detection Using CNNDocument16 pagesLiver Cancer Detection Using CNNSanjana NPas encore d'évaluation
- Hepatocellular CarcinomaDocument45 pagesHepatocellular Carcinomamhean azneitaPas encore d'évaluation
- Immune Mechanisms Linking Metabolic Injury To in Ammation and Fibrosis in Fatty Liver Disease - Novel Insights Into Cellular Communication CircuitsDocument25 pagesImmune Mechanisms Linking Metabolic Injury To in Ammation and Fibrosis in Fatty Liver Disease - Novel Insights Into Cellular Communication Circuitsdr. Nur'aini HasanPas encore d'évaluation
- Final 2021 Benefit Year Final HHS Risk Adjustment Model CoefficientsDocument26 pagesFinal 2021 Benefit Year Final HHS Risk Adjustment Model CoefficientsJ CHANGPas encore d'évaluation
- OST Clinical Medicine For The MRCP PACES Volume 1 PDFDocument607 pagesOST Clinical Medicine For The MRCP PACES Volume 1 PDFMOWNIAN100% (2)
- Chronic Liver DiseaseDocument12 pagesChronic Liver DiseaseamitPas encore d'évaluation
- Alcoholic Liver DiseasesDocument45 pagesAlcoholic Liver DiseasesSunith KanakuntlaPas encore d'évaluation
- Cirrhosis Patient Education 2014Document3 pagesCirrhosis Patient Education 2014Robert G. Gish, MDPas encore d'évaluation
- Beyond The Liver Function Tests: A Radiologist's Guide To The Liver Blood TestsDocument18 pagesBeyond The Liver Function Tests: A Radiologist's Guide To The Liver Blood Tests李冠Pas encore d'évaluation
- Cholestasis Is The Main Determinant of Abnormal CA 19-9 Levels in Patients With Liver CirrhosisDocument5 pagesCholestasis Is The Main Determinant of Abnormal CA 19-9 Levels in Patients With Liver CirrhosisPrima IncorynaPas encore d'évaluation
- The Ultimate Synergy Against Cancer: Fucoidan and AHCCDocument98 pagesThe Ultimate Synergy Against Cancer: Fucoidan and AHCCDr. Susana Trujillo100% (2)
- Drug Induced Liver DisordersDocument31 pagesDrug Induced Liver DisordersJason fernandes jPas encore d'évaluation
- Zhang 2013Document10 pagesZhang 2013Budi Utami FahnunPas encore d'évaluation
- PathoLOGY MCQDocument67 pagesPathoLOGY MCQHUSAMPas encore d'évaluation
- Cirse 2015 2015 PDFDocument324 pagesCirse 2015 2015 PDFEghar EverydayishellPas encore d'évaluation
- Chirosis Hepatic PDFDocument8 pagesChirosis Hepatic PDFCikalHrPas encore d'évaluation
- Telmisartan與失智的發生風險:全人口世代研究Document10 pagesTelmisartan與失智的發生風險:全人口世代研究Hima HuPas encore d'évaluation
- Nuclear MedicineDocument7 pagesNuclear MedicineMarco Mendoza67% (3)
- 3D NLS Grafiy EngDocument64 pages3D NLS Grafiy Engmedellincolombia100% (1)
- HBV EASL CPG Slide Deck 2020Document48 pagesHBV EASL CPG Slide Deck 2020Ajeng TunjungputriPas encore d'évaluation
- Clinical Significance of METTL Family Molecules in Hepatocellular CarcinomaDocument17 pagesClinical Significance of METTL Family Molecules in Hepatocellular CarcinomaSabrina JonesPas encore d'évaluation