Vous aimerez peut-être aussi
- Neurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesD'EverandNeurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesPas encore d'évaluation
- 07 PtosisDocument25 pages07 PtosisAndriani Kemala SariPas encore d'évaluation
- Classification of Ptosis: 1. NeurogenicDocument25 pagesClassification of Ptosis: 1. NeurogenicMuliany PratiwiPas encore d'évaluation
- MeningiomaDocument51 pagesMeningiomaarushijha2000Pas encore d'évaluation
- Optic NeuritisDocument31 pagesOptic NeuritisUsman ImtiazPas encore d'évaluation
- Eyelids Diseases Lacrimal System DiseasesDocument45 pagesEyelids Diseases Lacrimal System DiseasesMAMA LALAPas encore d'évaluation
- Thyroid Eye Disease: DR Aleena ShahDocument33 pagesThyroid Eye Disease: DR Aleena ShahhamsPas encore d'évaluation
- Double Vision / Diplopia: Dr. R. Handoko Pratomo, SPMDocument94 pagesDouble Vision / Diplopia: Dr. R. Handoko Pratomo, SPMNefri TiawarmanPas encore d'évaluation
- 30secondary GlaucomasDocument15 pages30secondary GlaucomasShari' Si WahyuPas encore d'évaluation
- 30secondary GlaucomasDocument19 pages30secondary GlaucomasShari' Si WahyuPas encore d'évaluation
- Embryologic DefectsDocument62 pagesEmbryologic DefectsBenjamin AgbonzePas encore d'évaluation
- Retina Nss2013Document46 pagesRetina Nss2013proluvieslacusPas encore d'évaluation
- 7 Peripheral Neuropathy MyopathyDocument83 pages7 Peripheral Neuropathy Myopathymuhammadridhwan100% (1)
- Dr. Bhosale SystemicDocument87 pagesDr. Bhosale SystemicdrksuhasPas encore d'évaluation
- Approach To A Case of DiplopiaDocument63 pagesApproach To A Case of DiplopiaSriniwasPas encore d'évaluation
- Thyroid Eye Disease: - Varshaa BDocument16 pagesThyroid Eye Disease: - Varshaa BRia SharmaPas encore d'évaluation
- 1400546814.1633unit 10 Nervous System PathophysiologyDocument27 pages1400546814.1633unit 10 Nervous System PathophysiologyRyan Adi PutraPas encore d'évaluation
- Developmental Disturbances of Oral Cavity-KushDocument405 pagesDevelopmental Disturbances of Oral Cavity-KushKush PathakPas encore d'évaluation
- PAED MicrocephalyDocument18 pagesPAED Microcephalyaboje ochekwuPas encore d'évaluation
- 6 - Intracranial MassDocument5 pages6 - Intracranial MassAmmarPas encore d'évaluation
- Eyedocs Excerpts PediatricsDocument14 pagesEyedocs Excerpts PediatricsMunib ur RehmanPas encore d'évaluation
- Thyroid OphthalmopathyDocument59 pagesThyroid OphthalmopathyLavanya MadabushiPas encore d'évaluation
- RADIOLOGI - NEURORADIOLOGI 2 - Dr. Farah - Kelas ADocument106 pagesRADIOLOGI - NEURORADIOLOGI 2 - Dr. Farah - Kelas ASeno TanubrataPas encore d'évaluation
- Slides For Pediatric Osce ExamDocument389 pagesSlides For Pediatric Osce Examadan yare100% (1)
- Pathology of The CnsDocument38 pagesPathology of The Cnscy lifePas encore d'évaluation
- Corneal DiseasesDocument32 pagesCorneal Diseasesnighat khanPas encore d'évaluation
- Grave'S Disease: Dr. Ibrahim, SPMDocument24 pagesGrave'S Disease: Dr. Ibrahim, SPMAnisa Karamina WardaniPas encore d'évaluation
- Multiple Sclerosis (Medicalstudyzone - Com)Document21 pagesMultiple Sclerosis (Medicalstudyzone - Com)WaleedPas encore d'évaluation
- Paediatric NeurophthalmologyDocument49 pagesPaediatric NeurophthalmologyNavami KrishnaPas encore d'évaluation
- Good MorningDocument76 pagesGood MorningCSE-A-2022-RAJESWARI NPas encore d'évaluation
- Menongioma PPT Slidshare PDFDocument75 pagesMenongioma PPT Slidshare PDFranggaPas encore d'évaluation
- Pupillary DisorderDocument19 pagesPupillary DisorderWan HafizPas encore d'évaluation
- Common Ocular DisordersDocument108 pagesCommon Ocular DisordersKa SalvinPas encore d'évaluation
- Diseases of Nerves and MusclesDocument46 pagesDiseases of Nerves and MusclesAME DENTAL COLLEGE RAICHUR, KARNATAKAPas encore d'évaluation
- Glaucoma and TinnitusDocument20 pagesGlaucoma and Tinnitusqurat-ul-ain.sonPas encore d'évaluation
- Neurocutaneous DisorderDocument20 pagesNeurocutaneous DisorderBarez AminPas encore d'évaluation
- DermatologyDocument223 pagesDermatologySahan EpitawalaPas encore d'évaluation
- Herpes Zoster: Bing-Rong ZHOUDocument43 pagesHerpes Zoster: Bing-Rong ZHOUMichael Jansen Sulaiman100% (1)
- Brain Tumor and Clinical FindingsDocument21 pagesBrain Tumor and Clinical FindingsAlbert Ciam100% (1)
- Neurocutaneous SyndromesDocument91 pagesNeurocutaneous SyndromesShakib ShafiPas encore d'évaluation
- MicrophtalmiaDocument5 pagesMicrophtalmiaMuhammad AdilPas encore d'évaluation
- Glaucoma & CataractDocument53 pagesGlaucoma & CataractBenita100% (1)
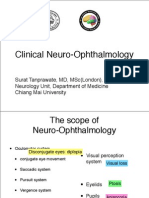
- Neuro Ophthalmology PDFDocument70 pagesNeuro Ophthalmology PDFSurat Tanprawate100% (4)
- Nervous System (S.S)Document112 pagesNervous System (S.S)Suman ShahPas encore d'évaluation
- 2019 Dr. Halida 1. Retinopati DiabetikafixDocument44 pages2019 Dr. Halida 1. Retinopati DiabetikafixLuthfia WardhaniPas encore d'évaluation
- Dermatology: Minci YazuminDocument48 pagesDermatology: Minci Yazuminminci senseiPas encore d'évaluation
- Trisomy 21-Down Syndrome: Payal DhakappaDocument35 pagesTrisomy 21-Down Syndrome: Payal DhakappaPayal AmarnathPas encore d'évaluation
- Disease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou UniversityDocument46 pagesDisease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou Universityapi-19916399Pas encore d'évaluation
- Semiology Lecture 4. Facies, Neck, ThyroidDocument59 pagesSemiology Lecture 4. Facies, Neck, ThyroidmlinaballerinaPas encore d'évaluation
- Complications of SinusitisDocument42 pagesComplications of SinusitisdrsadafrafiPas encore d'évaluation
- Neuritis OpticDocument13 pagesNeuritis OpticBimo Nugroho saktiPas encore d'évaluation
- Retinal Disorders Med VDocument66 pagesRetinal Disorders Med Vhenok birukPas encore d'évaluation
- Facial PalsyDocument25 pagesFacial PalsyMahad abuukarPas encore d'évaluation
- Optic Disc: Symptoms of The Optic Nerve DiseasesDocument11 pagesOptic Disc: Symptoms of The Optic Nerve DiseasesDilawar JanPas encore d'évaluation
- Diseases of Endocrine SystemDocument84 pagesDiseases of Endocrine SystemDuaa The PandaPas encore d'évaluation
- Facial PalsyDocument33 pagesFacial PalsyArista SPas encore d'évaluation
- Overview of Pediatric GeneticsDocument12 pagesOverview of Pediatric Geneticsnicdeep100% (1)
- Motor Neuron DiseaseDocument23 pagesMotor Neuron DiseaseNaman MishraPas encore d'évaluation
- Ptosis 03presenDocument26 pagesPtosis 03presentotalrevoltPas encore d'évaluation
- Adl IadlDocument20 pagesAdl IadlKrisna Eka Yudha100% (1)
- Maintaining Body AlignmentDocument6 pagesMaintaining Body AlignmentJan Jamison ZuluetaPas encore d'évaluation
- Cerebrovascular Accident CVADocument8 pagesCerebrovascular Accident CVAFlora Angeli PastoresPas encore d'évaluation
- Some Techniques To Remember The Names of MedicinesDocument6 pagesSome Techniques To Remember The Names of MedicinesGajanan NaikPas encore d'évaluation
- NCP Alleine PregnantDocument2 pagesNCP Alleine PregnantAlleine YvethPas encore d'évaluation
- 47 Case ReportDocument4 pages47 Case Reportsusanti bulanPas encore d'évaluation
- Pediatric Basic Life SupportDocument50 pagesPediatric Basic Life SupportnurmauliarizkyPas encore d'évaluation
- Correlation Between Healthcare Service Quality and HIV Testing Services Patient's Satisfaction in Kedungdoro Primary Health Care SurabayaDocument4 pagesCorrelation Between Healthcare Service Quality and HIV Testing Services Patient's Satisfaction in Kedungdoro Primary Health Care SurabayaAgung KatritamaPas encore d'évaluation
- Definition/Description: Types of SyringomyeliaDocument8 pagesDefinition/Description: Types of SyringomyeliaNurfadiyah YasinPas encore d'évaluation
- CBT Case SummaryDocument4 pagesCBT Case SummaryEva GonsherPas encore d'évaluation
- Protandim Summary of Clinincal Studies - University Version.Document3 pagesProtandim Summary of Clinincal Studies - University Version.ProtandimFanPas encore d'évaluation
- Anatomy of The KidneyDocument7 pagesAnatomy of The KidneyArgie Arguson IIPas encore d'évaluation
- Pediatrics Block 1Document258 pagesPediatrics Block 1Ghada ElhassanPas encore d'évaluation
- FessDocument3 pagesFessMadMariPas encore d'évaluation
- H02E Assignment 8Document4 pagesH02E Assignment 8Good ChannelPas encore d'évaluation
- Boy: - 2. Bus: - 3. Box: - 4. Mouse: - 5. Child: - 6. BabyDocument3 pagesBoy: - 2. Bus: - 3. Box: - 4. Mouse: - 5. Child: - 6. BabyMurni Abu BakarPas encore d'évaluation
- TITLE-class Diagram For Hospital Management SystemDocument2 pagesTITLE-class Diagram For Hospital Management SystemShivam JhaPas encore d'évaluation
- Secondary SurveyDocument2 pagesSecondary SurveySakta SuryagunaPas encore d'évaluation
- Therapeutic CommunicationDocument82 pagesTherapeutic CommunicationYvette Vallejo100% (2)
- Final Exam: Theory of Nursing SystemsDocument2 pagesFinal Exam: Theory of Nursing SystemsXeian Calamba RafaelPas encore d'évaluation
- NHS Pilots in Primary Care AnDocument8 pagesNHS Pilots in Primary Care AnAli RazaPas encore d'évaluation
- Suggamadex Remifentanyl PalonosetronDocument28 pagesSuggamadex Remifentanyl PalonosetronSai TejeswiPas encore d'évaluation
- Stage 1 Visit 1Document15 pagesStage 1 Visit 1amritakhatra7Pas encore d'évaluation
- Nur 129 Exam 2Document4 pagesNur 129 Exam 2Stephanie DuvergePas encore d'évaluation
- CAD/CAM Dentistry and Chairside Digital Impression Making: 4 CE CreditsDocument11 pagesCAD/CAM Dentistry and Chairside Digital Impression Making: 4 CE CreditsShraddha AgarwalPas encore d'évaluation
- WCU NURS 491L - Integration of Nursing Practice - 2014fall - I - 8-4-14Document29 pagesWCU NURS 491L - Integration of Nursing Practice - 2014fall - I - 8-4-14Joseph MeyerPas encore d'évaluation
- Comparison of UMN & LMN SyndromesDocument2 pagesComparison of UMN & LMN SyndromesPJHGPas encore d'évaluation
- Acute and Chronic Gastritis Due To Helicobacter PyloriDocument8 pagesAcute and Chronic Gastritis Due To Helicobacter PyloriCarla HolandPas encore d'évaluation
- Practical Standard Prescriber, 7th EditionDocument505 pagesPractical Standard Prescriber, 7th EditionTonyScaria60% (5)
- Anatomy of The Human Airways. Lymph Node Stations and InterventionalDocument6 pagesAnatomy of The Human Airways. Lymph Node Stations and Interventionalandika pradanaPas encore d'évaluation