Vous aimerez peut-être aussi
- Simphysis Pubis Disruption.Document36 pagesSimphysis Pubis Disruption.victorone22Pas encore d'évaluation
- Aniglide Plating of The Fibula.Document13 pagesAniglide Plating of The Fibula.victorone22Pas encore d'évaluation
- Anterograde Itramedulary Nailing.Document40 pagesAnterograde Itramedulary Nailing.victorone22Pas encore d'évaluation
- PatellaDocument31 pagesPatellavictorone22Pas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Lecture 2 - OsteologyDocument66 pagesLecture 2 - OsteologyRubia Iftikhar100% (1)
- Frequently Missed Fractures in Pediatric TraumaDocument13 pagesFrequently Missed Fractures in Pediatric Traumaalejasuarez248Pas encore d'évaluation
- Anatomy of The Peripheral Vascular System - 2Document34 pagesAnatomy of The Peripheral Vascular System - 2Perven Ganason100% (2)
- Ortopedia en AvesDocument14 pagesOrtopedia en AvesNatalia Gutiérrez100% (1)
- External Fixation of FemurDocument27 pagesExternal Fixation of FemurMemoona AmeerPas encore d'évaluation
- The Osteology of The Lower LimbDocument4 pagesThe Osteology of The Lower LimbAldi PrawidyaPas encore d'évaluation
- Amputation: Sites of Amputation: UEDocument6 pagesAmputation: Sites of Amputation: UEChristine PilarPas encore d'évaluation
- Osteology of The Lower LimbDocument4 pagesOsteology of The Lower LimbDungani AllanPas encore d'évaluation
- Journal of Orthopaedic Surgery and ResearchDocument6 pagesJournal of Orthopaedic Surgery and ResearchDewye SartikaPas encore d'évaluation
- Name of Muscle Origin Insertion Nerve Supply Action Muscles of The ThoraxDocument8 pagesName of Muscle Origin Insertion Nerve Supply Action Muscles of The ThoraxGabriel Angelo GuilasPas encore d'évaluation
- Anthrompometric Data Table PDFDocument1 pageAnthrompometric Data Table PDFRazero4Pas encore d'évaluation
- Pelvis (Summary)Document6 pagesPelvis (Summary)Michaella SangcapPas encore d'évaluation
- Dead LiftsDocument8 pagesDead LiftsjwarswolvesPas encore d'évaluation
- Anatomy Questions Hip and ThighDocument11 pagesAnatomy Questions Hip and Thighmohamed mowafeyPas encore d'évaluation
- Nexgen Lps Flex Fixed Bearing Knee Surgical TechniqueDocument24 pagesNexgen Lps Flex Fixed Bearing Knee Surgical TechniqueLenci MuratiPas encore d'évaluation
- EMG Placement TutorialDocument24 pagesEMG Placement TutorialAndrea Spencer100% (1)
- Catalago Final OsteoamericaDocument62 pagesCatalago Final OsteoamericaMaritza ArroyoPas encore d'évaluation
- Knee Anatomy and InjuriesDocument120 pagesKnee Anatomy and Injurieserfan mohammadi100% (2)
- Bandaging 130430003026 Phpapp02Document48 pagesBandaging 130430003026 Phpapp02Aruel Diano100% (1)
- Buku-Anatomi Osteologi PDFDocument56 pagesBuku-Anatomi Osteologi PDFmuhammad firdausPas encore d'évaluation
- XX Popliteal Fossa and Knee JointDocument43 pagesXX Popliteal Fossa and Knee JointAlistair WalkerPas encore d'évaluation
- Score PG GuideDocument389 pagesScore PG GuideAravindh SellaPas encore d'évaluation
- A Body, A Dog and A Fistful of ScatsDocument4 pagesA Body, A Dog and A Fistful of ScatsNoelle SpitzPas encore d'évaluation
- Basic OsteotomyDocument2 pagesBasic OsteotomyMichael JohnPas encore d'évaluation
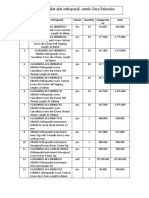
- List Pengajuan Asist Device Alat Orthopaedi Untuk GazaDocument5 pagesList Pengajuan Asist Device Alat Orthopaedi Untuk GazaRyantino IrdanPas encore d'évaluation
- Case Study ON Tibial Fracture: University of Saint LouisDocument50 pagesCase Study ON Tibial Fracture: University of Saint LouisJM RomiasPas encore d'évaluation
- Prevention of Legg-Calve-Perthes DiseaseDocument12 pagesPrevention of Legg-Calve-Perthes DiseaseNuno Craveiro LopesPas encore d'évaluation
- Femur Fracture Tie-In Fixation in A Dog - A Case ReportDocument3 pagesFemur Fracture Tie-In Fixation in A Dog - A Case ReportHari Krishna Nunna V VPas encore d'évaluation
- Appendicular SkeletonDocument65 pagesAppendicular Skeletonnanak00ciaraPas encore d'évaluation
- Normal Sizes and Other Aids (Radiology)Document16 pagesNormal Sizes and Other Aids (Radiology)nmb1986Pas encore d'évaluation