Vous aimerez peut-être aussi
- Esophageal Cancer, A Simple Guide To The Condition, Diagnosis And TreatmentD'EverandEsophageal Cancer, A Simple Guide To The Condition, Diagnosis And TreatmentPas encore d'évaluation
- Penis Cancer, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandPenis Cancer, A Simple Guide To The Condition, Treatment And Related ConditionsPas encore d'évaluation
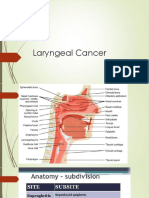
- Laryngeal Cancer 1Document49 pagesLaryngeal Cancer 1Kpj KpjPas encore d'évaluation
- Oropharyngeal CancerDocument4 pagesOropharyngeal CancerRusman Hadi RachmanPas encore d'évaluation
- Ovarian Cancer, A Simple Guide To The Condition, Diagnosis, TreatmentD'EverandOvarian Cancer, A Simple Guide To The Condition, Diagnosis, TreatmentPas encore d'évaluation
- Oncology NotesDocument7 pagesOncology NotesRochel Mae LomedaPas encore d'évaluation
- Chapter IDocument11 pagesChapter ISeptian RahaPas encore d'évaluation
- Particular Cancer Power PointDocument101 pagesParticular Cancer Power PointKoRnflakesPas encore d'évaluation
- Cervical CancerDocument7 pagesCervical CancerLarisse de LeonPas encore d'évaluation
- Lesson Plan On TumorsDocument19 pagesLesson Plan On TumorsPuneetPas encore d'évaluation
- Nursing Care Plan For Laryngeal Cancer - LifenursesDocument6 pagesNursing Care Plan For Laryngeal Cancer - LifenursesMădălina Pinciuc100% (2)
- Reproductive System Cancers by EasterDocument19 pagesReproductive System Cancers by EasterIGA ABRAHAM100% (1)
- What Is Breast CancerDocument4 pagesWhat Is Breast CancerRj RiosPas encore d'évaluation
- For Lung CancerDocument6 pagesFor Lung CancerMichael Jerome Parallag100% (3)
- Stomach CancerDocument7 pagesStomach CancerSyazmin KhairuddinPas encore d'évaluation
- NCP For Laryngeal CancerDocument5 pagesNCP For Laryngeal CancerMădălina PinciucPas encore d'évaluation
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Cervical Cancer: By. Ms. MurtiningsihDocument30 pagesCervical Cancer: By. Ms. MurtiningsihraiPas encore d'évaluation
- Print ONCODocument8 pagesPrint ONCOBJ DUQUESAPas encore d'évaluation
- Anal Cancer, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandAnal Cancer, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- gr.5 Colorectal CancerDocument9 pagesgr.5 Colorectal Cancerkeithlynd100% (1)
- Casestudy Gastric CarcinomaDocument53 pagesCasestudy Gastric CarcinomaAngelaTrinidadPas encore d'évaluation
- Cancer of THE Esophagus: Jevanette A. Velacruz BSN 3-B Group 2 NCM 116 RleDocument10 pagesCancer of THE Esophagus: Jevanette A. Velacruz BSN 3-B Group 2 NCM 116 RleVanetPas encore d'évaluation
- Colorectal CancerDocument3 pagesColorectal CancerAriane May Rubio50% (2)
- Ovarian CancerDocument15 pagesOvarian CancerAlmasPas encore d'évaluation
- Case Study: - Courtney ChaneyDocument29 pagesCase Study: - Courtney Chaneyapi-313356122Pas encore d'évaluation
- Ovarian Cancer 22Document15 pagesOvarian Cancer 22Irfan KhanPas encore d'évaluation
- Ca Stomach 01Document9 pagesCa Stomach 01MS AntikaPas encore d'évaluation
- Breast Cervical Cancer ManuscriptDocument9 pagesBreast Cervical Cancer ManuscriptRICHEVIN DENSOPas encore d'évaluation
- Vdocuments - MX Biology Investigatory Project Class Xii Breast CancerDocument14 pagesVdocuments - MX Biology Investigatory Project Class Xii Breast CancerPooja TikaniaPas encore d'évaluation
- Cervical CancerDocument28 pagesCervical CancerAmlan jyoti thanapatiPas encore d'évaluation
- CA EsophagusDocument101 pagesCA EsophagusMannuel TuttuPas encore d'évaluation
- Oral CancerDocument11 pagesOral CancerJils SureshPas encore d'évaluation
- Esophageal CancerDocument24 pagesEsophageal CancerSarah GatuzPas encore d'évaluation
- Cervical CancerDocument7 pagesCervical CancerChristine Joy Clemente BerjaPas encore d'évaluation
- Cancer of The UterusDocument5 pagesCancer of The UterusShreyas WalvekarPas encore d'évaluation
- Oncology NursingDocument21 pagesOncology NursingAqib SatarPas encore d'évaluation
- Breast Cancer Is The Most Common Invasive Cancer in Women, and The Second MainDocument4 pagesBreast Cancer Is The Most Common Invasive Cancer in Women, and The Second MainRaidis PangilinanPas encore d'évaluation
- Symptoms: Definition of Cervical Cancer: Cancer That Forms in Tissues of The Cervix (The Organ Connecting The UterusDocument5 pagesSymptoms: Definition of Cervical Cancer: Cancer That Forms in Tissues of The Cervix (The Organ Connecting The UterusHazel Joy Hokson-DiazPas encore d'évaluation
- Group 9 Ovarian and Uterine CancerDocument45 pagesGroup 9 Ovarian and Uterine CancerShiangPas encore d'évaluation
- Bladder CancerDocument27 pagesBladder Cancerabdoelshafey777Pas encore d'évaluation
- Cell Ab ActivitiesDocument7 pagesCell Ab ActivitiesJanelle Cabida Supnad100% (1)
- CASE ANALYSIS - Nasopharyngeal CancerDocument8 pagesCASE ANALYSIS - Nasopharyngeal CancerTerry Mae Atilazal SarciaPas encore d'évaluation
- Esophageal CancerDocument4 pagesEsophageal CancerhilcontiongsonPas encore d'évaluation
- Gi Ca, Nephroblastoma, Retinoblastoma, Skin Ca - Adavan, Gallardo, LeeDocument35 pagesGi Ca, Nephroblastoma, Retinoblastoma, Skin Ca - Adavan, Gallardo, LeeYzel Vasquez AdavanPas encore d'évaluation
- Cervical CancerDocument12 pagesCervical CancerMarylynn AmpofoPas encore d'évaluation
- Nursing OncologyDocument83 pagesNursing OncologyAndrea Huecas TriaPas encore d'évaluation
- Esophageal Cancer InserviceDocument18 pagesEsophageal Cancer Inserviceapi-371785797Pas encore d'évaluation
- 77case StudyDocument3 pages77case StudyTiffany AdriasPas encore d'évaluation
- Casestudy Gastric CarcinomaDocument56 pagesCasestudy Gastric CarcinomaMJ Amarillo92% (12)
- Breast CancersDocument9 pagesBreast CancersMS AntikaPas encore d'évaluation
- 3 NCM+116n+Lecture+Care+of+the+Clients+with+Problems+GI+Function+and+NutritionDocument4 pages3 NCM+116n+Lecture+Care+of+the+Clients+with+Problems+GI+Function+and+NutritionKylle AlimosaPas encore d'évaluation
- Competency Appraisal II: Lung/Bronchogenic CancerDocument7 pagesCompetency Appraisal II: Lung/Bronchogenic CancerArnie Jude CaridoPas encore d'évaluation
- Colorectal CancerDocument29 pagesColorectal CancerLeeyanBhadzzVagayPas encore d'évaluation
- Lung Cancer, A Simple Guide To The Cancer, Types And TreatmentsD'EverandLung Cancer, A Simple Guide To The Cancer, Types And TreatmentsPas encore d'évaluation
- CA MGTDocument114 pagesCA MGTMademoiselle KayettyPas encore d'évaluation
- Colon, Rectum and Anus-Dr. SigitDocument121 pagesColon, Rectum and Anus-Dr. SigitYuliana Latif100% (1)
- Case Personal CA MAMMAEDocument15 pagesCase Personal CA MAMMAEAdhitya Soewadji MartodimuljoPas encore d'évaluation
- Cancer of The Larynx 3Document15 pagesCancer of The Larynx 3Sahr Anne Pilar B. ParreñoPas encore d'évaluation
- Our Lady of Fatima University #1 Esperanza St. Hilltop MansionDocument6 pagesOur Lady of Fatima University #1 Esperanza St. Hilltop Mansionjames garciaPas encore d'évaluation
- ECG: Reading The WavesDocument9 pagesECG: Reading The Wavesjames garciaPas encore d'évaluation
- Anthony P. Toledo, MD, RNDocument30 pagesAnthony P. Toledo, MD, RNjames garcia100% (1)
- Pulmonary Edema: (Acute Heart Failure)Document7 pagesPulmonary Edema: (Acute Heart Failure)james garcia100% (5)
- LeukemiaDocument26 pagesLeukemiaKoRnflakes100% (1)
- Mammography (Breast X-Ray, Mammogram)Document2 pagesMammography (Breast X-Ray, Mammogram)james garciaPas encore d'évaluation
- Pneumothorax (Collapsed Lung)Document34 pagesPneumothorax (Collapsed Lung)james garcia100% (3)
- Fluid and ElectrolytesDocument52 pagesFluid and Electrolytesjames garciaPas encore d'évaluation
- Most Uterine Cancer Are Endometrioid (That Is, Originating in TheDocument5 pagesMost Uterine Cancer Are Endometrioid (That Is, Originating in Thejames garciaPas encore d'évaluation
- Cardio SystemDocument45 pagesCardio Systemapi-3735995100% (2)
- 3 Most Common Site of New Cancer Cases and Deaths in The United StatesDocument21 pages3 Most Common Site of New Cancer Cases and Deaths in The United Statesjames garciaPas encore d'évaluation
- Fluid and Electrolytes, Burns, G.U.Document56 pagesFluid and Electrolytes, Burns, G.U.james garciaPas encore d'évaluation
- CA ParticularsDocument101 pagesCA Particularsjames garciaPas encore d'évaluation
- CA StomachDocument6 pagesCA Stomachjames garciaPas encore d'évaluation
- Cancer of The Bladder and KidneyDocument8 pagesCancer of The Bladder and Kidneyjames garciaPas encore d'évaluation
- Breast CancerDocument32 pagesBreast Cancerjames garcia100% (1)
- Cardiac DysrythmiasDocument27 pagesCardiac DysrythmiasKoRnflakes100% (4)
- B Io CrisisDocument242 pagesB Io Crisisjames garciaPas encore d'évaluation
- ElectrocardiogramDocument16 pagesElectrocardiogramjames garciaPas encore d'évaluation
- Cancer of The Stomach and LiverDocument8 pagesCancer of The Stomach and Liverjames garciaPas encore d'évaluation
- Related Topics-Aneurysms EtcDocument23 pagesRelated Topics-Aneurysms Etcjames garciaPas encore d'évaluation
- Breast CancerDocument32 pagesBreast Cancerjames garcia100% (1)
- Assessment and DX of CancerDocument6 pagesAssessment and DX of Cancerjames garciaPas encore d'évaluation
- Dka He Esrd Ards PoisoningDocument29 pagesDka He Esrd Ards Poisoningjames garciaPas encore d'évaluation
- CARE Management Lecture 8 - Cellular Abbe RationsDocument15 pagesCARE Management Lecture 8 - Cellular Abbe Rationsjames garciaPas encore d'évaluation
- Finals Ms2Document324 pagesFinals Ms2james garciaPas encore d'évaluation
- Burns and ShockDocument13 pagesBurns and Shockjames garciaPas encore d'évaluation
- Our Lady of Fatima UniversityDocument13 pagesOur Lady of Fatima Universityjames garciaPas encore d'évaluation
- CARDIOVERSION Vs DEFIBRILLATIONDocument7 pagesCARDIOVERSION Vs DEFIBRILLATIONjames garciaPas encore d'évaluation
- Đề Thi Tủ Pte Helper 2Document52 pagesĐề Thi Tủ Pte Helper 2Văn Hữu ĐạtPas encore d'évaluation
- Taylan Competency NeedsDocument32 pagesTaylan Competency NeedsLovejoice Cha NnelPas encore d'évaluation
- Visa Application FAQ-SummerDocument8 pagesVisa Application FAQ-SummerCaioAndradePas encore d'évaluation
- Foss L.-The End of Modern Medicine. Biomedical Science Under A Microscope-State Univ. of NY (2002) PDFDocument352 pagesFoss L.-The End of Modern Medicine. Biomedical Science Under A Microscope-State Univ. of NY (2002) PDFSusi RutmalemPas encore d'évaluation
- ProposalDocument41 pagesProposalMark B. BarrogaPas encore d'évaluation
- Apply Appropriate Safety Measures While Working inDocument28 pagesApply Appropriate Safety Measures While Working inNanette A. Marañon-Sansano100% (5)
- MSDS-Muriate of Potash 2017Document11 pagesMSDS-Muriate of Potash 2017Inoe69Pas encore d'évaluation
- Proposal For The BoosterDocument5 pagesProposal For The BoosterraziPas encore d'évaluation
- A Triumph of Surgery A Triumph of SurgeryDocument7 pagesA Triumph of Surgery A Triumph of SurgeryAmol PagarePas encore d'évaluation
- Internet Addiction - ResearchDocument13 pagesInternet Addiction - ResearchpipedsPas encore d'évaluation
- Closure MineDocument14 pagesClosure MineAmilton filhoPas encore d'évaluation
- Logic ModelDocument2 pagesLogic ModelstojannaPas encore d'évaluation
- SF2 Aquarius Set BDocument2 pagesSF2 Aquarius Set BXyzaPas encore d'évaluation
- Toxoplasmosis Serologic Testing AlgorithmDocument1 pageToxoplasmosis Serologic Testing AlgorithmHanny Prasetiana YuriantiPas encore d'évaluation
- Laporan IKM KSM PK FEBRUARI 2022Document28 pagesLaporan IKM KSM PK FEBRUARI 2022Nur iffahPas encore d'évaluation
- Nursing Care Plan 2 Knowledge DeficitDocument7 pagesNursing Care Plan 2 Knowledge Deficitdbryant0101100% (3)
- MalariaDocument170 pagesMalariatummalapalli venkateswara rao100% (4)
- Diary Card Sample 04Document3 pagesDiary Card Sample 04MaryPas encore d'évaluation
- BKV Application Form (Sea Staff) Rev08Document5 pagesBKV Application Form (Sea Staff) Rev08Mehmet ErgeanPas encore d'évaluation
- Covid Test-PositiveDocument2 pagesCovid Test-PositiveSuresh VarmaPas encore d'évaluation
- FeverDocument2 pagesFeverMuhammad Jefri LukmanPas encore d'évaluation
- FDP Form 7 - 20% Component of The IRA Utilization 20% Component of The Ira Utilization For The First Quarter, Cy 2017Document32 pagesFDP Form 7 - 20% Component of The IRA Utilization 20% Component of The Ira Utilization For The First Quarter, Cy 2017Juna Majistad CrismundoPas encore d'évaluation
- RULE 1142. Marine Tank Vessel OperationsDocument8 pagesRULE 1142. Marine Tank Vessel OperationsksalvaradoPas encore d'évaluation
- P CLS14 Powertec Compact Leg Sled ManualDocument15 pagesP CLS14 Powertec Compact Leg Sled ManualElizabeth GuzmanPas encore d'évaluation
- Walk or Cycle For 'A Happier Commute': BBC Learning English Words in The NewsDocument2 pagesWalk or Cycle For 'A Happier Commute': BBC Learning English Words in The NewsCaio Augusto Takaki UechiPas encore d'évaluation
- Hazmat Transportation Training RequirementsDocument12 pagesHazmat Transportation Training RequirementsSafety IezzproPas encore d'évaluation
- Combine PDFDocument164 pagesCombine PDFmichael.quintanaPas encore d'évaluation
- MoH - Uganda RBF Program Hospital Quartely Quality Assessment Tool - Jan 2019Document31 pagesMoH - Uganda RBF Program Hospital Quartely Quality Assessment Tool - Jan 2019Steven SsemwangaPas encore d'évaluation
- Anatomi Dan Fisiologi Mata 1Document61 pagesAnatomi Dan Fisiologi Mata 1MAWANPas encore d'évaluation
- Birthday Party - Character SketchesDocument2 pagesBirthday Party - Character SketchesDhivyaPas encore d'évaluation