Vous aimerez peut-être aussi
- Transposition of The Great Arteries: Eric Osborn January 27, 2010Document35 pagesTransposition of The Great Arteries: Eric Osborn January 27, 2010Soad ShedeedPas encore d'évaluation
- Transposition of Great ArteriesDocument21 pagesTransposition of Great ArteriesAlusio Navosailagi VUNIIVI100% (1)
- Congenital Heart Diseases: Charles University of Prague 2 Faculty of Medicine Filip KoubekDocument43 pagesCongenital Heart Diseases: Charles University of Prague 2 Faculty of Medicine Filip KoubekAdel HamzicPas encore d'évaluation
- Complete Transposition of Great ArteriesDocument85 pagesComplete Transposition of Great ArteriesRahul AgrawalPas encore d'évaluation
- Congenital Heart Disease For The Adult Cardiologist: Transposition of The Great ArteriesDocument12 pagesCongenital Heart Disease For The Adult Cardiologist: Transposition of The Great ArteriesSaid hanPas encore d'évaluation
- Penyakit Katup Jantung-Kuliah DR ErlinaDocument70 pagesPenyakit Katup Jantung-Kuliah DR ErlinaAdhiatma DotPas encore d'évaluation
- Adult Congenital Heart Disease Board ReviewDocument79 pagesAdult Congenital Heart Disease Board ReviewKhajornsak Som-UnPas encore d'évaluation
- Cyanotic Heart DiseaseDocument66 pagesCyanotic Heart DiseasePrasanth SankarPas encore d'évaluation
- Duct Dependent Lesions - PPSXDocument41 pagesDuct Dependent Lesions - PPSXSindujaPas encore d'évaluation
- Penyakit Jantung KongenitalDocument30 pagesPenyakit Jantung KongenitalrintiikPas encore d'évaluation
- Adult Congenital Heart Disease Board ReviewDocument76 pagesAdult Congenital Heart Disease Board ReviewOQAB13Pas encore d'évaluation
- Penyakit Katup Jantung: Dr. Tjatur Winarsanto SPPD Rs CiremaiDocument59 pagesPenyakit Katup Jantung: Dr. Tjatur Winarsanto SPPD Rs CiremaianisamayaPas encore d'évaluation
- Microsoft PowerPoint - ECHOCARDIOGRAPHY IN ADULT CONGENITAL HEART DISEASE PDFDocument51 pagesMicrosoft PowerPoint - ECHOCARDIOGRAPHY IN ADULT CONGENITAL HEART DISEASE PDFHanafieHeluthPas encore d'évaluation
- Congenital Heart Diseases : CyanoticDocument25 pagesCongenital Heart Diseases : CyanoticVignaa PrashanthPas encore d'évaluation
- Congenital Heart Disease EtiologyDocument8 pagesCongenital Heart Disease EtiologykudzaimuregidubePas encore d'évaluation
- Cctga PcicsDocument9 pagesCctga PcicsAdrian KhomanPas encore d'évaluation
- 14 Clauss Pediatric Echocardiography PDFDocument159 pages14 Clauss Pediatric Echocardiography PDFSergiu NiculitaPas encore d'évaluation
- Transposition of Great Artery: 1. AbstractDocument7 pagesTransposition of Great Artery: 1. AbstractA. Fajar AprianiPas encore d'évaluation
- Tricuspid Atresia VivekDocument66 pagesTricuspid Atresia VivekIlham FatthurPas encore d'évaluation
- Transposition of The Great Arteries PDFDocument6 pagesTransposition of The Great Arteries PDFSakuntalaPalanki100% (2)
- Cyanosis in The NewbornDocument32 pagesCyanosis in The Newbornimma_2014Pas encore d'évaluation
- Aortic Stenosis AmendillaDocument31 pagesAortic Stenosis AmendillaVadim BursacovschiPas encore d'évaluation
- TOF Patient EducationDocument8 pagesTOF Patient EducationMia MiaPas encore d'évaluation
- Tips and Tricks in Management of Patients With CHDDocument46 pagesTips and Tricks in Management of Patients With CHDDrMarcus KeyboardPas encore d'évaluation
- Cvs-k7-Valvular Heart Disease Nora2010Document52 pagesCvs-k7-Valvular Heart Disease Nora2010shiloinPas encore d'évaluation
- Cyanotic Congenital Heart DiseaseDocument8 pagesCyanotic Congenital Heart DiseaseMohammed Taha Al-nuaimyPas encore d'évaluation
- Rheumatic Heart DiseaseDocument47 pagesRheumatic Heart DiseaseGideon K. MutaiPas encore d'évaluation
- Congenital Heart DeseasesDocument54 pagesCongenital Heart DeseasesAntony100% (1)
- Congenital Heart DefectsDocument73 pagesCongenital Heart DefectsStaen KisPas encore d'évaluation
- Tetralogy of FallotDocument5 pagesTetralogy of FallotSaloni MehtaPas encore d'évaluation
- The Adult Fontan PatientDocument31 pagesThe Adult Fontan PatientAnonymous p1lonwiCDFPas encore d'évaluation
- Cyanotic Congenital Heart DiseaseDocument22 pagesCyanotic Congenital Heart DiseaseRaviPas encore d'évaluation
- What Is Tetralogy of FallotDocument18 pagesWhat Is Tetralogy of FallotIyah Bu-ucanPas encore d'évaluation
- Congenital Heart Disease: Kevin Jones Senior Chief Technician Alder Hey Childrens HospitalDocument32 pagesCongenital Heart Disease: Kevin Jones Senior Chief Technician Alder Hey Childrens HospitalVaibhav KaroliyaPas encore d'évaluation
- Acn U# 3Document21 pagesAcn U# 3Kamran AltafPas encore d'évaluation
- PJB Pada Dewasa AASDocument54 pagesPJB Pada Dewasa AAS1e23e2ewPas encore d'évaluation
- Cardiac Outflow Tract TableDocument3 pagesCardiac Outflow Tract TableCathyCluverPas encore d'évaluation
- Valvular Heart DiseaseDocument10 pagesValvular Heart DiseaseEzyan SyaminPas encore d'évaluation
- Transposition of Great Vessels (Tga) : Thottempudi TejaDocument8 pagesTransposition of Great Vessels (Tga) : Thottempudi TejaVenkat Sai GadiparthiPas encore d'évaluation
- Cyanotic Congenital Heart DiseaseDocument50 pagesCyanotic Congenital Heart DiseaseSasi KumarPas encore d'évaluation
- Tetralogy of FallotDocument3 pagesTetralogy of FallotKamal FauzePas encore d'évaluation
- Tetralogy of Fallot PDFDocument11 pagesTetralogy of Fallot PDFIma SoniaPas encore d'évaluation
- Tricuspid AtresiaDocument44 pagesTricuspid Atresiadoctorsaty7539Pas encore d'évaluation
- TUGAS Ventricular Septal DefectDocument8 pagesTUGAS Ventricular Septal DefectMohammad NafisPas encore d'évaluation
- Tricuspid Atresia VivekDocument66 pagesTricuspid Atresia Vivekmihalcea alin100% (1)
- Hollamby Mitchell s5001226 Case 1 DtgaDocument13 pagesHollamby Mitchell s5001226 Case 1 Dtgaapi-299009880Pas encore d'évaluation
- Amboss:CardioDocument18 pagesAmboss:CardioNicole Juliette CCPas encore d'évaluation
- Tetralogy of FallotDocument31 pagesTetralogy of FallotDevipriya MajumderPas encore d'évaluation
- Congenital Heart DiseaseDocument10 pagesCongenital Heart DiseaseIca JustitiaPas encore d'évaluation
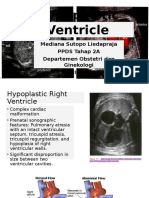
- Hypoplastic Ventricle. MEDIDocument21 pagesHypoplastic Ventricle. MEDIBenny Franclin SuripattyPas encore d'évaluation
- Practice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaDocument28 pagesPractice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaRully SyahrizalPas encore d'évaluation
- Peds Shelf NotesDocument74 pagesPeds Shelf NotesRandy BornmannPas encore d'évaluation
- Neonatal CardiologyDocument35 pagesNeonatal CardiologyCiopraga IuliaPas encore d'évaluation
- Transposition of The Great ArteriesDocument29 pagesTransposition of The Great ArteriesbookwormMD100% (1)
- Congenital Heart Diseases: Non Cyanotic PlethoraDocument43 pagesCongenital Heart Diseases: Non Cyanotic PlethoraFauzi SatriaPas encore d'évaluation
- Atrial Flutter EmedicineDocument8 pagesAtrial Flutter EmedicineErnis Wahyu OktianaPas encore d'évaluation
- Electrocardiograms in The Pediatric EDDocument69 pagesElectrocardiograms in The Pediatric EDbradsoboPas encore d'évaluation
- Knapp TestDocument2 pagesKnapp TestGeorge Litu67% (3)
- Esok RPHDocument1 pageEsok RPHAzira RoshanPas encore d'évaluation
- Remo Vs DevanaderaDocument2 pagesRemo Vs DevanaderaZymon Andrew MaquintoPas encore d'évaluation
- Coaching Skills For Optimal PerformanceDocument58 pagesCoaching Skills For Optimal PerformanceYodhia Antariksa100% (3)
- ABHI Network List As On 30-06-2023Document3 401 pagesABHI Network List As On 30-06-20233uifbcsktPas encore d'évaluation
- Florentino Vs EncarnacionDocument2 pagesFlorentino Vs EncarnacionJay Mark Esconde50% (2)
- Government of Kerala: Minority CertificateDocument1 pageGovernment of Kerala: Minority CertificateBI185824125 Personal AccountingPas encore d'évaluation
- Lara CroftDocument58 pagesLara CroftMarinko Tikvicki67% (3)
- Assignment 1 TVM, Bonds StockDocument2 pagesAssignment 1 TVM, Bonds StockMuhammad Ali SamarPas encore d'évaluation
- Musical Rhythm, Linguistic Rhythm, and Human EvolutionDocument7 pagesMusical Rhythm, Linguistic Rhythm, and Human Evolutiongeneup3587100% (1)
- Ipsoot Rating ClarificationsDocument9 pagesIpsoot Rating ClarificationsJerry PanPas encore d'évaluation
- Chapter 1 (Research)Document6 pagesChapter 1 (Research)Salome CarpioPas encore d'évaluation
- MKTG How Analytics Can Drive Growth in Consumer Packaged Goods Trade PromotionsDocument5 pagesMKTG How Analytics Can Drive Growth in Consumer Packaged Goods Trade PromotionsCultura AnimiPas encore d'évaluation
- Thermal ComfortDocument6 pagesThermal ComfortHoucem Eddine MechriPas encore d'évaluation
- Hermeneutical Phenomenology and Human Enviroment SystemDocument12 pagesHermeneutical Phenomenology and Human Enviroment SystemAllen Rose Buenaflor BuenoPas encore d'évaluation
- Emcee - Graduation DayDocument5 pagesEmcee - Graduation DayBharanisri VeerendiranPas encore d'évaluation
- Revision Notes On Section 1.6 - Belief, Uncertainty & UnbeliefDocument5 pagesRevision Notes On Section 1.6 - Belief, Uncertainty & Unbeliefnisalielisha rodrigoPas encore d'évaluation
- Managing Individual Differences and BehaviorDocument40 pagesManaging Individual Differences and BehaviorDyg Norjuliani100% (1)
- Agreement - AFS - RERA Punjab 20190906pro - Forma - Agreement - of - Sale - To - Be - Signed - With - AllotteesDocument35 pagesAgreement - AFS - RERA Punjab 20190906pro - Forma - Agreement - of - Sale - To - Be - Signed - With - AllotteesPuran Singh LabanaPas encore d'évaluation
- TPTG620 Bc200412615: Assignment 2 (Week 2)Document12 pagesTPTG620 Bc200412615: Assignment 2 (Week 2)afia afiaPas encore d'évaluation
- Pro Angular JS (Apress)Document1 pagePro Angular JS (Apress)Dreamtech PressPas encore d'évaluation
- HeavyReding ReportDocument96 pagesHeavyReding ReportshethPas encore d'évaluation
- NUR 200 Week 7 Practice Case StudyDocument2 pagesNUR 200 Week 7 Practice Case StudyJB NicolePas encore d'évaluation
- Cayman Islands National Youth Policy September 2000Document111 pagesCayman Islands National Youth Policy September 2000Kyler GreenwayPas encore d'évaluation
- WE) The Accentual Structure of English WordsDocument8 pagesWE) The Accentual Structure of English Wordszhannatagabergen2606Pas encore d'évaluation
- Conspicuous Consumption-A Literature ReviewDocument15 pagesConspicuous Consumption-A Literature Reviewlieu_hyacinthPas encore d'évaluation
- Wardancer 4e HomebrewDocument3 pagesWardancer 4e HomebrewWyjecPas encore d'évaluation
- Projectile Motion PhysicsDocument3 pagesProjectile Motion Physicsapi-325274340Pas encore d'évaluation
- The American New CriticsDocument5 pagesThe American New CriticsSattigul KharakozhaPas encore d'évaluation
- Associate-Shopping in Hyderabad, Telangana Careers at HyderabadDocument1 pageAssociate-Shopping in Hyderabad, Telangana Careers at HyderabadpavanPas encore d'évaluation