Vous aimerez peut-être aussi
- Blood and Cell Physiology MCQs With KeyDocument9 pagesBlood and Cell Physiology MCQs With KeyMudassar Roomi88% (64)
- MCQs On Respiration Physiology With KeyDocument7 pagesMCQs On Respiration Physiology With KeyMudassar Roomi94% (31)
- MCQs On Circulation Physiology With KeyDocument6 pagesMCQs On Circulation Physiology With KeyMudassar Roomi91% (34)
- Hematology NotesDocument4 pagesHematology NotesHannah Grace CorveraPas encore d'évaluation
- Histology & Cell BiologyDocument33 pagesHistology & Cell BiologyMohSen100% (1)
- Lecture 1 Blood Physiology by Dr. RoomiDocument24 pagesLecture 1 Blood Physiology by Dr. RoomiMudassar Roomi75% (4)
- Namita JaggiDocument4 pagesNamita JaggiIJAMPas encore d'évaluation
- HB Synthesis, Degradation, Jaundice, Iron Metabolism by Dr. RoomiDocument23 pagesHB Synthesis, Degradation, Jaundice, Iron Metabolism by Dr. RoomiMudassar Roomi100% (1)
- CBC Reviewer Anaphy LabDocument9 pagesCBC Reviewer Anaphy LabARVINE JUSTINE CORPUZPas encore d'évaluation
- BLOOD Physiology Guyton 14th Edition Chapter 33Document57 pagesBLOOD Physiology Guyton 14th Edition Chapter 33Dr Alamzeb Jadoon100% (1)
- RBC MembraneDocument41 pagesRBC MembranemwambungupPas encore d'évaluation
- Autoimmune Hemolytic AnemiaDocument55 pagesAutoimmune Hemolytic AnemiaNicky SebastianPas encore d'évaluation
- 4 - HemoglobinopathiesDocument19 pages4 - HemoglobinopathiesHamzehPas encore d'évaluation
- Lecture On Hemostasis by Dr. RoomiDocument43 pagesLecture On Hemostasis by Dr. RoomiMudassar Roomi100% (1)
- HAEMOPOIESISDocument6 pagesHAEMOPOIESISDiyana ZahariPas encore d'évaluation
- Pathophysiology PCP 341: Nermien Waly MD, M.SC., PH.DDocument48 pagesPathophysiology PCP 341: Nermien Waly MD, M.SC., PH.DBalsam Zahi Al-HasanPas encore d'évaluation
- Haem MCQ 2012 Student Feedback PDFDocument18 pagesHaem MCQ 2012 Student Feedback PDFaminata6Pas encore d'évaluation
- Blood Components Where Do They Come From?: Introduction To HaematologyDocument11 pagesBlood Components Where Do They Come From?: Introduction To Haematologydorsa koraeiPas encore d'évaluation
- Hematology 1 Quiz 2 3Document27 pagesHematology 1 Quiz 2 3Jam Ramos100% (1)
- Physiology of Skeletal Muscle by Dr. RoomiDocument33 pagesPhysiology of Skeletal Muscle by Dr. RoomiMudassar RoomiPas encore d'évaluation
- ABO Blood GroupsDocument18 pagesABO Blood GroupsRamadan PhysiologyPas encore d'évaluation
- Hemopoiesis PDFDocument14 pagesHemopoiesis PDFrysnawahyu13Pas encore d'évaluation
- Blood ComponentDocument17 pagesBlood ComponentJes CmtPas encore d'évaluation
- Haemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)Document20 pagesHaemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)shravaniPas encore d'évaluation
- Microscopic ExaminationDocument72 pagesMicroscopic ExaminationbubblyeivinejPas encore d'évaluation
- Haematology - Blood Films.Document6 pagesHaematology - Blood Films.kkkssbb100% (1)
- Wintrobe Test PDFDocument9 pagesWintrobe Test PDFMaria Chacón CarbajalPas encore d'évaluation
- S0850alug 1670953860959-SEU HDocument56 pagesS0850alug 1670953860959-SEU HAziz KhwajaPas encore d'évaluation
- HaematologyDocument68 pagesHaematologytapoolnoPas encore d'évaluation
- Blood 12-6-2018Document42 pagesBlood 12-6-2018Noor Fatima100% (1)
- RH Blood Group SystemDocument6 pagesRH Blood Group SystemUsman ChPas encore d'évaluation
- CBCDocument12 pagesCBCDaNa Al-jomah100% (1)
- Automation in HaematologyDocument67 pagesAutomation in Haematologyk11a1r18Pas encore d'évaluation
- ErythropoiesisDocument51 pagesErythropoiesisKevin Leo100% (1)
- Physiology, Lecture 4, Blood (Slides)Document28 pagesPhysiology, Lecture 4, Blood (Slides)Ali Al-QudsiPas encore d'évaluation
- Blood ComponentsDocument17 pagesBlood ComponentsJohnSmithPas encore d'évaluation
- Hematology 1 Lab - The Reticulocyte CountDocument17 pagesHematology 1 Lab - The Reticulocyte CountCIRILO MABBORANGPas encore d'évaluation
- Hematology BMLS 103Document88 pagesHematology BMLS 103harpreetPas encore d'évaluation
- RBC Production and DestructionDocument44 pagesRBC Production and DestructionNehemiah FranciscoPas encore d'évaluation
- Microcytic Hypochromic Anemia: - M QariDocument33 pagesMicrocytic Hypochromic Anemia: - M QarirohitPas encore d'évaluation
- PlateletsDocument23 pagesPlateletsnirilibPas encore d'évaluation
- Immune Response ClassDocument55 pagesImmune Response ClassKoushali BanerjeePas encore d'évaluation
- Neutrophils: in Health and DiseaseDocument65 pagesNeutrophils: in Health and DiseaseKush Pathak100% (1)
- RBC IndicesDocument13 pagesRBC IndicespremPas encore d'évaluation
- Introduction To HematologyDocument23 pagesIntroduction To HematologyReba PhiliposePas encore d'évaluation
- Blood Grouping ReagentsDocument7 pagesBlood Grouping ReagentsDominic EmerencianaPas encore d'évaluation
- Blood Grouping and Crosss MatchingDocument39 pagesBlood Grouping and Crosss MatchingDr. Pawan KumarPas encore d'évaluation
- Manual Platelet CountDocument14 pagesManual Platelet CountMiyo SobremisanaPas encore d'évaluation
- 1 Edited My Class Note 1 On Blood BankDocument42 pages1 Edited My Class Note 1 On Blood Bankmatewos100% (1)
- Antibodies Structure and FunctionDocument16 pagesAntibodies Structure and Functionياسين احمد علي الشيخPas encore d'évaluation
- Blood, Coagulation of Blood & Bleeding Disorders 12 - 7 - 19Document62 pagesBlood, Coagulation of Blood & Bleeding Disorders 12 - 7 - 19AntarleenaPas encore d'évaluation
- 1 Renal FunctionDocument5 pages1 Renal FunctionChristopher BucuPas encore d'évaluation
- NERVE & MUSCLE 45 Qs With Their Answer Keys by Dr. RoomiDocument54 pagesNERVE & MUSCLE 45 Qs With Their Answer Keys by Dr. RoomiMudassar Roomi100% (1)
- CML, CLLDocument118 pagesCML, CLLMunesh SherawatPas encore d'évaluation
- Haem. Notes (MBCHB) ProperDocument162 pagesHaem. Notes (MBCHB) ProperKelvinTMaikanaPas encore d'évaluation
- ABO Blood Group System. LegitDocument11 pagesABO Blood Group System. LegitShestrelmay Launico UmingaPas encore d'évaluation
- Anatomy and Physiology, Heart, BP and Hematology Labs MoodleDocument70 pagesAnatomy and Physiology, Heart, BP and Hematology Labs MoodleLeena LapenaPas encore d'évaluation
- Anemia Its Laboratory DiagnosisDocument146 pagesAnemia Its Laboratory DiagnosisCh M MushahidPas encore d'évaluation
- HemostasisDocument48 pagesHemostasissianturisuryaPas encore d'évaluation
- Pathology of Blood and Lymphatic VesselsDocument55 pagesPathology of Blood and Lymphatic VesselsMhinory OctPas encore d'évaluation
- Lecture 1 Physiology of Skeletal Muscle by Dr. RoomiDocument37 pagesLecture 1 Physiology of Skeletal Muscle by Dr. RoomiMudassar Roomi100% (1)
- Hematology QuestionsDocument171 pagesHematology QuestionsVikkineshwaran Siva SubramaniamPas encore d'évaluation
- CLINICAL CHEMISTRY: Passbooks Study GuideD'EverandCLINICAL CHEMISTRY: Passbooks Study GuidePas encore d'évaluation
- 4th Lecture On Arrythmias by Dr. RoomiDocument11 pages4th Lecture On Arrythmias by Dr. RoomiMudassar Roomi100% (2)
- Lecture On Basics of ECG For 1st Year MBBS by Dr. RoomiDocument28 pagesLecture On Basics of ECG For 1st Year MBBS by Dr. RoomiMudassar Roomi100% (3)
- Physiology of Excitation and Conduction System of Heart by Dr. Mudassar Ali RoomiDocument17 pagesPhysiology of Excitation and Conduction System of Heart by Dr. Mudassar Ali RoomiMudassar Roomi100% (1)
- 3rd Lecture On Arrythmias by Dr. RoomiDocument16 pages3rd Lecture On Arrythmias by Dr. RoomiMudassar Roomi100% (2)
- GIT Physiology CHAPTER NO 62 Guyton by Dr. RoomiDocument41 pagesGIT Physiology CHAPTER NO 62 Guyton by Dr. RoomiMudassar Roomi86% (14)
- Lecture On Hemostasis by Dr. RoomiDocument43 pagesLecture On Hemostasis by Dr. RoomiMudassar Roomi100% (1)
- 1st Lec On Heart Physiology by Dr. RoomiDocument21 pages1st Lec On Heart Physiology by Dr. RoomiMudassar RoomiPas encore d'évaluation
- Lecture 3 Skeletal Muscle Physiology by Dr. RoomiDocument10 pagesLecture 3 Skeletal Muscle Physiology by Dr. RoomiMudassar Roomi100% (1)
- Lecture 3 Skeletal Muscle Physiology by Dr. RoomiDocument10 pagesLecture 3 Skeletal Muscle Physiology by Dr. RoomiMudassar Roomi100% (1)
- Key of SEQs Heart, Nerve and Muscle Revision TestDocument11 pagesKey of SEQs Heart, Nerve and Muscle Revision TestMudassar Roomi100% (2)
- 3rd Lecture On Arrythmias by Dr. RoomiDocument16 pages3rd Lecture On Arrythmias by Dr. RoomiMudassar Roomi100% (2)
- Lecture On Anemias and Polycythemias by Dr. RoomiDocument30 pagesLecture On Anemias and Polycythemias by Dr. RoomiMudassar Roomi100% (1)
- Lecture 1 Physiology of Skeletal Muscle by Dr. RoomiDocument37 pagesLecture 1 Physiology of Skeletal Muscle by Dr. RoomiMudassar Roomi100% (1)
- Lecture On The Physiology of Hypothalamus and Thalamus by Dr. RoomiDocument27 pagesLecture On The Physiology of Hypothalamus and Thalamus by Dr. RoomiMudassar Roomi100% (1)
- Lecture On Basal Ganglia by Dr. RoomiDocument32 pagesLecture On Basal Ganglia by Dr. RoomiMudassar Roomi100% (3)
- 2nd Lecture On Skeletal Muscle Physiology by Dr. Mudassar Ali RoomiDocument29 pages2nd Lecture On Skeletal Muscle Physiology by Dr. Mudassar Ali RoomiMudassar Roomi100% (1)
- Lecture On The Physiology of Neuromuscular Junction (NMJ) by Dr. RoomiDocument18 pagesLecture On The Physiology of Neuromuscular Junction (NMJ) by Dr. RoomiMudassar Roomi100% (3)
- Sense of Touch - Practical by Dr. RoomiDocument14 pagesSense of Touch - Practical by Dr. RoomiMudassar RoomiPas encore d'évaluation
- Lecture On PHYSIOLOGY of Cerebellum by Dr. RoomiDocument42 pagesLecture On PHYSIOLOGY of Cerebellum by Dr. RoomiMudassar Roomi100% (2)
- Lecture Synapses, Properties & Transmission Dr. RoomiDocument22 pagesLecture Synapses, Properties & Transmission Dr. RoomiMudassar Roomi100% (2)
- Heart, Nerve and Mucsle, Membrane Transport Mcqs With KeyDocument8 pagesHeart, Nerve and Mucsle, Membrane Transport Mcqs With KeyMudassar Roomi100% (7)
- Physiology of Limbic System by Dr. RoomiDocument18 pagesPhysiology of Limbic System by Dr. RoomiMudassar Roomi50% (2)
- Blood and Cell Physiology SEQs KeyDocument11 pagesBlood and Cell Physiology SEQs KeyMudassar Roomi100% (1)
- Respiration Physiology SEQs With KeyDocument12 pagesRespiration Physiology SEQs With KeyMudassar Roomi100% (1)
- Circulation SEQs With KeysDocument15 pagesCirculation SEQs With KeysMudassar Roomi100% (1)
- Alpha ThalassemiaDocument31 pagesAlpha ThalassemiaBen SabladaPas encore d'évaluation
- History, Introduction & Scope of MicrbiologyDocument13 pagesHistory, Introduction & Scope of MicrbiologyKazi TanimPas encore d'évaluation
- Blood TranfusionDocument18 pagesBlood TranfusionVishnu PriyaPas encore d'évaluation
- Blood Grouping and Cross MatchingDocument2 pagesBlood Grouping and Cross MatchinganupreetPas encore d'évaluation
- Atlas Medical BacteriologyDocument104 pagesAtlas Medical BacteriologyradulusPas encore d'évaluation
- Influenza - AiniDocument11 pagesInfluenza - AiniAl- ImanuddinPas encore d'évaluation
- CH 01 The Microbial WorldDocument21 pagesCH 01 The Microbial Worldsammy alan0% (1)
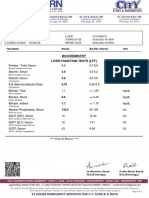
- Biochemistry Liver Function Tests (LFT)Document1 pageBiochemistry Liver Function Tests (LFT)Rohit JunejaPas encore d'évaluation
- PHVT Food Microbiology PDFDocument35 pagesPHVT Food Microbiology PDFAzianuPas encore d'évaluation
- Classification and Indentification of BacteriaDocument77 pagesClassification and Indentification of BacteriaAnand MadhavanPas encore d'évaluation
- RH NegativeDocument3 pagesRH NegativeChelzie LasernaPas encore d'évaluation
- Blood Banking: Donor ScreeningDocument16 pagesBlood Banking: Donor ScreeningNikka Ong100% (2)
- The Red Cell Histogram and The Dimorphic Red Cell PopulationDocument9 pagesThe Red Cell Histogram and The Dimorphic Red Cell PopulationAlan Dwi SaputraPas encore d'évaluation
- RH Blood Group SystemDocument12 pagesRH Blood Group SystemRohailPas encore d'évaluation
- Microbial Limit Test by Pour Plate MethodDocument25 pagesMicrobial Limit Test by Pour Plate MethodAnkit Verma100% (4)
- Reading Activit Level 1 Semester 1Document3 pagesReading Activit Level 1 Semester 1ghaleb alhaidaryPas encore d'évaluation
- Blood Componant Therapy (Autosaved)Document47 pagesBlood Componant Therapy (Autosaved)drkapiltPas encore d'évaluation
- Bailey Scott's Diagnostic Microbiolog13th Ed (Dragged) 2Document1 pageBailey Scott's Diagnostic Microbiolog13th Ed (Dragged) 2Reg LagartejaPas encore d'évaluation
- V 5 N 1Document190 pagesV 5 N 1Jorge RodriguezPas encore d'évaluation
- Dapus MakalahDocument2 pagesDapus MakalahAndra NurjayaPas encore d'évaluation
- Centro Escolar University Makati Campus Department of Nursing 2 SEM 2019-2020 BSN 2asDocument2 pagesCentro Escolar University Makati Campus Department of Nursing 2 SEM 2019-2020 BSN 2asmyeonniePas encore d'évaluation
- Kidd Blood Group SystemDocument6 pagesKidd Blood Group SystemMuhammad FirdausPas encore d'évaluation
- Certificate of Completion STDDocument3 pagesCertificate of Completion STDapi-415083061Pas encore d'évaluation
- Blood Transfusion PDFDocument7 pagesBlood Transfusion PDFBaboolal100% (2)
- Git Pathogenic BacteriaDocument12 pagesGit Pathogenic BacteriaAnnisaa FitrianiPas encore d'évaluation
- DIAGNOSTICS (Student Copy)Document59 pagesDIAGNOSTICS (Student Copy)Abigail Mayled LausPas encore d'évaluation
- ICD 10 - Chapter 1 Certain Infectious and Parasitic DiseasesDocument16 pagesICD 10 - Chapter 1 Certain Infectious and Parasitic DiseasesHuseikha VelayazulfahdPas encore d'évaluation
- Nilai Rujukan Hematologi AnakDocument6 pagesNilai Rujukan Hematologi AnakirdinamarchsyaPas encore d'évaluation
- K.Hema Anandhy, M.SC Nursing, PuducherryDocument53 pagesK.Hema Anandhy, M.SC Nursing, PuducherryhemihemaPas encore d'évaluation