Vous aimerez peut-être aussi
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisD'EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- Thermal Analysis V2: Inorganic Materials and Physical ChemistryD'EverandThermal Analysis V2: Inorganic Materials and Physical ChemistryRobert F. Jr. SchwenkerÉvaluation : 1 sur 5 étoiles1/5 (1)
- Jurnal Penatalaksanaan EdemaDocument7 pagesJurnal Penatalaksanaan EdemaMariska Nada Debora100% (1)
- EritrositDocument12 pagesEritrositNatasya HerinPas encore d'évaluation
- at Ast Tgo IfccDocument2 pagesat Ast Tgo IfccNisrinaPas encore d'évaluation
- Prinsip Poct Dan Faktor Yang Mempengaruhi Hasil Poct FinalDocument33 pagesPrinsip Poct Dan Faktor Yang Mempengaruhi Hasil Poct Finalahmad syaifulPas encore d'évaluation
- Alkaline Phosphatase: Colorimetric MethodDocument2 pagesAlkaline Phosphatase: Colorimetric MethodFariz KasyidiPas encore d'évaluation
- Sintesis DNADocument32 pagesSintesis DNAZhafran DarwisPas encore d'évaluation
- Pemeriksaan Fungsi Hati, DR - DiahDocument42 pagesPemeriksaan Fungsi Hati, DR - DiahYuliana LatifPas encore d'évaluation
- The Cardiovascular System: The Heart: AnatomyDocument62 pagesThe Cardiovascular System: The Heart: AnatomyLingga GumelarPas encore d'évaluation
- Na2B4O7 PDFDocument5 pagesNa2B4O7 PDFmariyana kusumawatiPas encore d'évaluation
- Genetika ManusiaDocument65 pagesGenetika Manusiadies100% (1)
- Spesifikasi TMS 24i Premium With Barcode System Without ISEDocument4 pagesSpesifikasi TMS 24i Premium With Barcode System Without ISEsky skyPas encore d'évaluation
- Assignment Of: Group VDocument13 pagesAssignment Of: Group VArslan Ejaz100% (1)
- PI e UREA 16Document2 pagesPI e UREA 16Moch Abdul RokimPas encore d'évaluation
- Jurnal GlikogenDocument6 pagesJurnal GlikogenChoirummintin Wa KhilafahPas encore d'évaluation
- Thrombotic Thrombocytopenic Purpura (TTP) : Rd. Kemas Diffa Zahputra. PKDocument11 pagesThrombotic Thrombocytopenic Purpura (TTP) : Rd. Kemas Diffa Zahputra. PKAnonymous cy6fLAPas encore d'évaluation
- AdrenalineDocument20 pagesAdrenalinecreatativePas encore d'évaluation
- Bilirubin Jendrassik-Grof FS Reagent R1 Sulphanilic Acid-Solution - En-GB-17Document9 pagesBilirubin Jendrassik-Grof FS Reagent R1 Sulphanilic Acid-Solution - En-GB-17Rahadian MahargiriPas encore d'évaluation
- Tutor Imun HBsAg KuantitatifDocument27 pagesTutor Imun HBsAg Kuantitatifv_mayasari100% (1)
- Acute Myeloid Leukemia With Myelodysplasia RelatedDocument6 pagesAcute Myeloid Leukemia With Myelodysplasia RelatedAgus WiniPas encore d'évaluation
- ID Ekspresi Dan Purifikasi Protein RekombinDocument12 pagesID Ekspresi Dan Purifikasi Protein RekombinRizQi FatmiyahPas encore d'évaluation
- Multiple Myeloma OverviewDocument52 pagesMultiple Myeloma OverviewanmegpraPas encore d'évaluation
- Jurnal - Komponen DarahDocument6 pagesJurnal - Komponen Darahvivi maykasariPas encore d'évaluation
- Jurnal Artikel Aau 1 PDFDocument7 pagesJurnal Artikel Aau 1 PDFRizkiSeptiaPas encore d'évaluation
- Natriuretic Peptide SystemDocument30 pagesNatriuretic Peptide SystemKhaled S. HarbPas encore d'évaluation
- Para Protein Emi ADocument14 pagesPara Protein Emi AMohamoud MohamedPas encore d'évaluation
- Jurnal Alkohol KualitatifDocument8 pagesJurnal Alkohol KualitatifMastuti Widi LestariPas encore d'évaluation
- Biuret TestDocument10 pagesBiuret TestJanine Vega Calayo100% (1)
- Ck-Nac: IFCC Single VialDocument2 pagesCk-Nac: IFCC Single VialFariz KasyidiPas encore d'évaluation
- Cysticercosis (Panneerselvam Gowtham 90A)Document13 pagesCysticercosis (Panneerselvam Gowtham 90A)Gautam Josh100% (1)
- Physioex Lab Report: Pre-Lab Quiz ResultsDocument4 pagesPhysioex Lab Report: Pre-Lab Quiz ResultsPavel MilenkovskiPas encore d'évaluation
- Biokimia 2 GLIKOLISISDocument18 pagesBiokimia 2 GLIKOLISISnamharPas encore d'évaluation
- SS Agar PronadisaDocument2 pagesSS Agar PronadisaMuhamad AfidinPas encore d'évaluation
- 5a. Mekanisme Imunitas Seluler Dan HumoralDocument32 pages5a. Mekanisme Imunitas Seluler Dan HumoralGaluh Apsari SyafranPas encore d'évaluation
- CRP Latex Package InsertDocument2 pagesCRP Latex Package InsertDaffa Samudera Nakz Doeratip100% (1)
- Insert Kit Uji NarkobaDocument2 pagesInsert Kit Uji NarkobaFatimah azzahraPas encore d'évaluation
- Laboratory Reference Ranges in Healthy Adults: ElectrolytesDocument2 pagesLaboratory Reference Ranges in Healthy Adults: ElectrolytesClauvinna Lie FiscaPas encore d'évaluation
- Boehm 1Document10 pagesBoehm 1Yolanda Priscilia GustantiaPas encore d'évaluation
- Pendukung Mikroalbuminuria, Kreatini, UcrDocument21 pagesPendukung Mikroalbuminuria, Kreatini, UcrHesty AshanPas encore d'évaluation
- Farmakokinetika Tugas Soal PPT EkstravaskulerDocument17 pagesFarmakokinetika Tugas Soal PPT Ekstravaskulertaka oneokrock18Pas encore d'évaluation
- Ca 19-9Document40 pagesCa 19-9Woro Hapsari WahyuningrumPas encore d'évaluation
- 3 Proteomics Tools and TechniquesDocument51 pages3 Proteomics Tools and TechniquesUmar JavedPas encore d'évaluation
- Enzymatic Creatinine: Reagent/ Product Code: Product Code: Product Code: Description Component 11420002 11420003 11420004Document2 pagesEnzymatic Creatinine: Reagent/ Product Code: Product Code: Product Code: Description Component 11420002 11420003 11420004غالب الموسويPas encore d'évaluation
- UrinalisisDocument81 pagesUrinalisisTitis CresnaulanPas encore d'évaluation
- Msds Lithium SulfateDocument6 pagesMsds Lithium SulfateLili RosePas encore d'évaluation
- HDL Precipitant 2Document7 pagesHDL Precipitant 2Nur IndahPas encore d'évaluation
- Kuliah Keseimbangan Asam BasaDocument38 pagesKuliah Keseimbangan Asam BasaSarah Lesty Adila100% (1)
- Sindrom KardiorenalDocument12 pagesSindrom KardiorenalAndreAHutasoitPas encore d'évaluation
- Chapter 1Document5 pagesChapter 1Christian EduardoPas encore d'évaluation
- Pemeriksaan HormonDocument91 pagesPemeriksaan HormonAdimas Ratmanhana KesumaPas encore d'évaluation
- Cytochemical StainDocument13 pagesCytochemical Staindreyngerous100% (4)
- CH 9 Protein Detection AnalysisDocument43 pagesCH 9 Protein Detection AnalysisYan XiongPas encore d'évaluation
- Lampiran 4 CLSIDocument4 pagesLampiran 4 CLSIRevina Ilka Busri SikumbangPas encore d'évaluation
- By M. J. Caldwell and D. B. Parrish (From The Kansas Agricultural Experiment Manhattan) (Received For Publication, December 26, 1944)Document7 pagesBy M. J. Caldwell and D. B. Parrish (From The Kansas Agricultural Experiment Manhattan) (Received For Publication, December 26, 1944)Indah WulansariPas encore d'évaluation
- Indrawati Et Al. (2019)Document5 pagesIndrawati Et Al. (2019)wahyu putri setiawatiPas encore d'évaluation
- Hemoglobin Opa ThiesDocument34 pagesHemoglobin Opa ThiesFebri fitraPas encore d'évaluation
- Daftar Harga Bahan Kimia Pada Aplikasi Supply Chain (Sucha)Document144 pagesDaftar Harga Bahan Kimia Pada Aplikasi Supply Chain (Sucha)Pace RaditPas encore d'évaluation
- (JDS) Journal of Syiah Kuala Dentistry SocietyDocument11 pages(JDS) Journal of Syiah Kuala Dentistry SocietyDindaPas encore d'évaluation
- BMA (Bone Marrow Aspiration)Document15 pagesBMA (Bone Marrow Aspiration)Ayu DewiPas encore d'évaluation
- Infeksi DR GdeDocument1 pageInfeksi DR Gdeflower boyPas encore d'évaluation
- Admin,+099+ +133+ +Ibnu+Purwanto+ +galleyDocument4 pagesAdmin,+099+ +133+ +Ibnu+Purwanto+ +galleyflower boyPas encore d'évaluation
- MurmursDocument14 pagesMurmursMartina RizkiPas encore d'évaluation
- HypertensionDocument52 pagesHypertensionpatriciajesikaPas encore d'évaluation
- Hubungan Veget Dengan Berat Badan Sama Prevalensi Diabetes 2Document6 pagesHubungan Veget Dengan Berat Badan Sama Prevalensi Diabetes 2flower boyPas encore d'évaluation
- Terapi Metabolik Menggunakan Diet VegetarianDocument4 pagesTerapi Metabolik Menggunakan Diet Vegetarianflower boyPas encore d'évaluation
- Health Effects of Vegan DietsDocument7 pagesHealth Effects of Vegan DietsAyrton SergeiPas encore d'évaluation
- Met VeganDocument4 pagesMet Veganflower boyPas encore d'évaluation
- PinkDocument1 pagePinkflower boyPas encore d'évaluation
- Faktor Resiko Metabolik Sindrom Terhadap VegetarianDocument3 pagesFaktor Resiko Metabolik Sindrom Terhadap Vegetarianflower boyPas encore d'évaluation
- VegansDocument8 pagesVeganswirajcomPas encore d'évaluation
- Hubungan Veget Dengan Berat Badan Sama Prevalensi Diabetes 2Document6 pagesHubungan Veget Dengan Berat Badan Sama Prevalensi Diabetes 2flower boyPas encore d'évaluation
- BesiDocument6 pagesBesiflower boyPas encore d'évaluation
- Journal of Nutrition College, Volume 1, Nomor 1, Tahun 2012, Halaman 63-71Document9 pagesJournal of Nutrition College, Volume 1, Nomor 1, Tahun 2012, Halaman 63-71flower boyPas encore d'évaluation
- Met VeganDocument4 pagesMet Veganflower boyPas encore d'évaluation
- Urology ExaminationDocument7 pagesUrology Examinationflower boyPas encore d'évaluation
- 10Document4 pages10flower boyPas encore d'évaluation
- PinkDocument1 pagePinkflower boyPas encore d'évaluation
- Blok Xiii: Uropoetika: Laporan Tutorial Skenario 3Document1 pageBlok Xiii: Uropoetika: Laporan Tutorial Skenario 3flower boyPas encore d'évaluation
- Sepsis and SIRSDocument24 pagesSepsis and SIRSFryda 'buona' YantiPas encore d'évaluation
- Cardiac Biomarker 2014Document41 pagesCardiac Biomarker 2014flower boyPas encore d'évaluation
- Pencegahan Peny Jantung Dan Pemb DarahDocument52 pagesPencegahan Peny Jantung Dan Pemb Darahflower boyPas encore d'évaluation
- Sepsis and SIRSDocument24 pagesSepsis and SIRSFryda 'buona' YantiPas encore d'évaluation
- Jadwal Kegiatan Blok 5 2013 100413Document7 pagesJadwal Kegiatan Blok 5 2013 100413flower boyPas encore d'évaluation
- Students Guidebook 2013 Blok5Document23 pagesStudents Guidebook 2013 Blok5flower boyPas encore d'évaluation
- Anemia Blok 6Document29 pagesAnemia Blok 6flower boyPas encore d'évaluation
- Psychoanalysis AND History: Freud: Dreaming, Creativity and TherapyDocument2 pagesPsychoanalysis AND History: Freud: Dreaming, Creativity and TherapyJuan David Millán MendozaPas encore d'évaluation
- Phardose Lab Prep 19 30Document4 pagesPhardose Lab Prep 19 30POMPEYO BARROGAPas encore d'évaluation
- READING 4 UNIT 8 Crime-Nurse Jorge MonarDocument3 pagesREADING 4 UNIT 8 Crime-Nurse Jorge MonarJORGE ALEXANDER MONAR BARRAGANPas encore d'évaluation
- Brody2012 PDFDocument13 pagesBrody2012 PDFfrancisca caceresPas encore d'évaluation
- Health Promotion Officers - CPD Booklet Schedule PDFDocument5 pagesHealth Promotion Officers - CPD Booklet Schedule PDFcharles KadzongaukamaPas encore d'évaluation
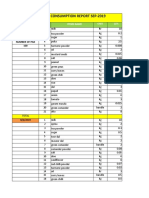
- Daily Staff Food Consumption Reports Sep-2019Document4 pagesDaily Staff Food Consumption Reports Sep-2019Manjit RawatPas encore d'évaluation
- Null 6 PDFDocument1 pageNull 6 PDFSimbarashe ChikariPas encore d'évaluation
- 5SDD 71B0210Document4 pages5SDD 71B0210Merter TolunPas encore d'évaluation
- Guideline On Smacna Through Penetration Fire StoppingDocument48 pagesGuideline On Smacna Through Penetration Fire Stoppingwguindy70Pas encore d'évaluation
- REV Description Appr'D CHK'D Prep'D: Tolerances (Unless Otherwise Stated) - (In)Document2 pagesREV Description Appr'D CHK'D Prep'D: Tolerances (Unless Otherwise Stated) - (In)Bacano CapoeiraPas encore d'évaluation
- Case Report CMV RetinitisDocument27 pagesCase Report CMV RetinitistaniamaulaniPas encore d'évaluation
- Solar Refrigeration: Prepared by M.DevakumarDocument21 pagesSolar Refrigeration: Prepared by M.DevakumarEasy StudyPas encore d'évaluation
- Entitlement Cure SampleDocument34 pagesEntitlement Cure SampleZondervan100% (1)
- Lab Manual PDFDocument68 pagesLab Manual PDFSantino AwetPas encore d'évaluation
- METHOD STATEMENT FOR INSTALLATION OF Light FixturesDocument5 pagesMETHOD STATEMENT FOR INSTALLATION OF Light FixturesNaveenPas encore d'évaluation
- Finite Element Analysis Project ReportDocument22 pagesFinite Element Analysis Project ReportsaurabhPas encore d'évaluation
- 107 2021 High Speed Rail Corridor RegDocument3 pages107 2021 High Speed Rail Corridor Rega siva sankarPas encore d'évaluation
- RRC Group D Notification 70812Document11 pagesRRC Group D Notification 70812admin2772Pas encore d'évaluation
- Eric Koech CV - Docx..bakDocument7 pagesEric Koech CV - Docx..bakPeter Osundwa KitekiPas encore d'évaluation
- EV Hammer Impact Crusher - ENDocument8 pagesEV Hammer Impact Crusher - ENKeshav NandaPas encore d'évaluation
- Neuro M Summary NotesDocument4 pagesNeuro M Summary NotesNishikaPas encore d'évaluation
- Penilaian Akhir TahunDocument4 pagesPenilaian Akhir TahunRestu Suci UtamiPas encore d'évaluation
- Rooftop Rain Water Harvesting in An Educational CampusDocument9 pagesRooftop Rain Water Harvesting in An Educational CampusAkshay BoratiPas encore d'évaluation
- BV Lesson Plan 4Document3 pagesBV Lesson Plan 4api-252119803Pas encore d'évaluation
- India Wine ReportDocument19 pagesIndia Wine ReportRajat KatiyarPas encore d'évaluation
- Cargador de BateríaDocument34 pagesCargador de BateríaBenPas encore d'évaluation
- UK Tax SystemDocument13 pagesUK Tax SystemMuhammad Sajid Saeed100% (1)
- Transfer and Business Taxation SyllabusDocument5 pagesTransfer and Business Taxation SyllabusamqqndeahdgePas encore d'évaluation
- Bai Tap Tieng Anh Lop 8 (Bai 13)Document4 pagesBai Tap Tieng Anh Lop 8 (Bai 13)nguyenanhmaiPas encore d'évaluation
- Present Continuous Exercises Test 1 - Positive Statements ExerciseDocument2 pagesPresent Continuous Exercises Test 1 - Positive Statements Exerciseangel omar peraltaPas encore d'évaluation