Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- 1 - Practice Test - CST 10th Grade ScienceDocument11 pages1 - Practice Test - CST 10th Grade Sciencefaithinhim7515Pas encore d'évaluation
- NP 3Document20 pagesNP 3MENARDPas encore d'évaluation
- Hema CA 1500Document4 pagesHema CA 1500Maya RustamPas encore d'évaluation
- Heart Failure With Reduced Ejection FractionDocument19 pagesHeart Failure With Reduced Ejection Fractiondussanjodo1497100% (2)
- Funcion Resp Senectud DR OyarzunDocument8 pagesFuncion Resp Senectud DR OyarzunPriscila Suazo CornejoPas encore d'évaluation
- Subclinical HypothyroidismDocument10 pagesSubclinical HypothyroidismRoberto López MataPas encore d'évaluation
- Alucinogenos y SuicidioDocument4 pagesAlucinogenos y Suicidiodussanjodo1497Pas encore d'évaluation
- Leptospirosis Vs DengueDocument5 pagesLeptospirosis Vs Denguedussanjodo1497Pas encore d'évaluation
- Leptospirosis Vs DengueDocument5 pagesLeptospirosis Vs Denguedussanjodo1497Pas encore d'évaluation
- OE Worksheet BASIC 0380Document6 pagesOE Worksheet BASIC 0380dussanjodo1497Pas encore d'évaluation
- Science Illustrated 60 - 2018 AUDocument84 pagesScience Illustrated 60 - 2018 AUCeleborn021Pas encore d'évaluation
- Atheism Is A Wrong Logic According To Islam 1Document3 pagesAtheism Is A Wrong Logic According To Islam 1Moh Andi KusumawardhanaPas encore d'évaluation
- BONAVERA CountDocument15 pagesBONAVERA CountpsychejanePas encore d'évaluation
- Haematology Test Result Unit Biological Ref. Interval Prothrombin TimeDocument6 pagesHaematology Test Result Unit Biological Ref. Interval Prothrombin TimeNidhi RakeshPas encore d'évaluation
- Bone Marrow Aspiration ThesisDocument5 pagesBone Marrow Aspiration Thesisfjf1y2rz100% (1)
- RBC, Structure and FunctionDocument17 pagesRBC, Structure and FunctionAsyha KantifaPas encore d'évaluation
- Life Processes Class XDocument3 pagesLife Processes Class XARYAN RAJPas encore d'évaluation
- Cause Dhemorragie Post Partum A Laquelle Il Faut Penser: Pseudo-Anevrisme de Lartere Uterine Apres Une Cesarienne, A Propos Dun CasDocument6 pagesCause Dhemorragie Post Partum A Laquelle Il Faut Penser: Pseudo-Anevrisme de Lartere Uterine Apres Une Cesarienne, A Propos Dun CasIJAR JOURNALPas encore d'évaluation
- Peripheral Blood SmearDocument46 pagesPeripheral Blood SmearAris ResurreccionPas encore d'évaluation
- Blood Gas MachineDocument33 pagesBlood Gas MachinenofearnofearPas encore d'évaluation
- Effects of SmokingDocument3 pagesEffects of SmokingKristine HeideePas encore d'évaluation
- EMG NotesDocument20 pagesEMG NotesArchit DasguptaPas encore d'évaluation
- Educational Manual Masterword SCD English FINALDocument111 pagesEducational Manual Masterword SCD English FINALbranchardmushabePas encore d'évaluation
- Reference Values For Common Laboratory Tests: Pharmacotherapy Self-Assessment ProgramDocument1 pageReference Values For Common Laboratory Tests: Pharmacotherapy Self-Assessment ProgramkatyPas encore d'évaluation
- Common Nursing AbbreviationsDocument8 pagesCommon Nursing AbbreviationsHana-Lou Taquiqui100% (1)
- AmpathDocument336 pagesAmpathHlulani DecisionPas encore d'évaluation
- An Introduction To The Human BodyDocument43 pagesAn Introduction To The Human BodySherleen Jane D. Fernandez50% (2)
- Scalar Energy Pendant / Quantum PendantDocument11 pagesScalar Energy Pendant / Quantum PendantDixon MailluPas encore d'évaluation
- Science 6 Living Things and Their Environment Earth and Space As Reviewed by SME 1Document36 pagesScience 6 Living Things and Their Environment Earth and Space As Reviewed by SME 1Elma Ortega CamionPas encore d'évaluation
- Product Abstracts: CMV & Pp65: (Ifa, Dfa, & Oligodetect®)Document17 pagesProduct Abstracts: CMV & Pp65: (Ifa, Dfa, & Oligodetect®)joseluisrodriguezvazquezPas encore d'évaluation
- Blood BookletDocument10 pagesBlood BookletTezdjan HassanPas encore d'évaluation
- Circulatory SystemDocument26 pagesCirculatory SystemCandyAnonymousPas encore d'évaluation
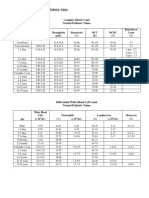
- 30a2131 Complete Blood Count Normal Pediatric Values PDFDocument1 page30a2131 Complete Blood Count Normal Pediatric Values PDFReziel Basilan Manalo100% (2)
- Frontier Foundation Welfare Hospital & Blood Transfusion Services ProfileDocument8 pagesFrontier Foundation Welfare Hospital & Blood Transfusion Services ProfileLaiba FayazPas encore d'évaluation
- 2007 Reference Range Book Nov 2007Document141 pages2007 Reference Range Book Nov 2007Wael AlkhiaryPas encore d'évaluation
- DR Katek BalapalaDocument73 pagesDR Katek BalapalaNathan LupiyaPas encore d'évaluation
- Your Amazing BodyDocument30 pagesYour Amazing Bodyj100% (1)