Vous aimerez peut-être aussi
- Posterior Polar Cataract Management: My Approach: 2022, #1D'EverandPosterior Polar Cataract Management: My Approach: 2022, #1Pas encore d'évaluation
- White Intumescent Cataract Management: My Approach: 2022, #1D'EverandWhite Intumescent Cataract Management: My Approach: 2022, #1Pas encore d'évaluation
- Sics Steps: Divisi Katarak Dan Bedah Refraktif Rumah Sakit Mata Bali MandaraDocument74 pagesSics Steps: Divisi Katarak Dan Bedah Refraktif Rumah Sakit Mata Bali MandaraPande GustianaPas encore d'évaluation
- Teknik Operasi KatarakDocument33 pagesTeknik Operasi KatarakD'Mhan MbozoPas encore d'évaluation
- Mecegah Komplikasi SicsDocument9 pagesMecegah Komplikasi Sicsinna_luv_u9006Pas encore d'évaluation
- PhacoemulsificationDocument54 pagesPhacoemulsificationIshita Kinra100% (1)
- Phco LectureDocument57 pagesPhco Lecturemedhanit anjuloPas encore d'évaluation
- Vitreous Prolapse ManagementDocument31 pagesVitreous Prolapse ManagementR.m. AndriyanPas encore d'évaluation
- Basic VitrectomyDocument24 pagesBasic Vitrectomykomitemedik.rsudsdaPas encore d'évaluation
- Nov 20: Journey in Neuroendoscopy: SinghDocument21 pagesNov 20: Journey in Neuroendoscopy: SinghAtharv SinghPas encore d'évaluation
- Eye ProblemsDocument25 pagesEye ProblemsHikmat UllahPas encore d'évaluation
- Cataract Surgery: Past-Present-FutureDocument44 pagesCataract Surgery: Past-Present-FutureNica Lopez FernandezPas encore d'évaluation
- CricothyroidotomyDocument41 pagesCricothyroidotomyNur SusiawantyPas encore d'évaluation
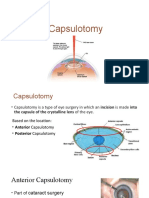
- CapsulotomyDocument15 pagesCapsulotomyAdrian PearlPas encore d'évaluation
- TrabeculectomyDocument42 pagesTrabeculectomyAnita Zhang100% (1)
- Surgical Management of Senile CataractDocument39 pagesSurgical Management of Senile CataractKarthik ChellaPas encore d'évaluation
- Spineinstrumentation 220325073013Document98 pagesSpineinstrumentation 220325073013Anwer YahyaPas encore d'évaluation
- Permanent Tunnel CatheterDocument52 pagesPermanent Tunnel CatheterJanice MuliadiPas encore d'évaluation
- ENT QuestionsDocument24 pagesENT QuestionsVijay BabuPas encore d'évaluation
- 3266 Small Incision Cataract Booklet Low ResDocument37 pages3266 Small Incision Cataract Booklet Low ResDiana NovacPas encore d'évaluation
- Why When and HowDocument11 pagesWhy When and Howamrit koiralaPas encore d'évaluation
- Oculofacial Plastic and Orbital SurgeryDocument14 pagesOculofacial Plastic and Orbital SurgeryTakwinPas encore d'évaluation
- Basics of Microvascular SurgeryDocument33 pagesBasics of Microvascular SurgeryPratikshya KothiaPas encore d'évaluation
- Gingivectomy & CurettageDocument55 pagesGingivectomy & CurettageRajani GedelaPas encore d'évaluation
- Eye ProsthesesDocument75 pagesEye ProsthesesNiharika SabharwalPas encore d'évaluation
- The Flap Technique For Pocket TherapyDocument34 pagesThe Flap Technique For Pocket TherapyNia Lieanto0% (1)
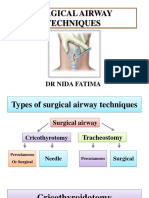
- Surgicalairwaytechniques 180526060828 PDFDocument72 pagesSurgicalairwaytechniques 180526060828 PDFWael ShamyPas encore d'évaluation
- ICP MonitoringDocument2 pagesICP MonitoringMandyAoPas encore d'évaluation
- Access Cavity PreparationDocument35 pagesAccess Cavity PreparationShaheen Aboobacker Reniya ShaheenPas encore d'évaluation
- Small Incision Cataract Surgery: Kumar Vaibhav 3 Year MD Ophthalmology Resident Bpklcos, TuthDocument67 pagesSmall Incision Cataract Surgery: Kumar Vaibhav 3 Year MD Ophthalmology Resident Bpklcos, TuthSriniwasPas encore d'évaluation
- Surgery of The EyeDocument3 pagesSurgery of The Eyehonovezaann.a.campita.ctucvmPas encore d'évaluation
- Insertion and Operation of IABP-1Document10 pagesInsertion and Operation of IABP-1Atia KiranPas encore d'évaluation
- ISMT 12 - Day 519 - Vito - Surgery For Epidural and Subdural HematomasDocument24 pagesISMT 12 - Day 519 - Vito - Surgery For Epidural and Subdural HematomasVito MasagusPas encore d'évaluation
- Neck DissectionDocument45 pagesNeck DissectionAbel AbrahamPas encore d'évaluation
- 3.2. ECMO Cannulation and PitfallDocument85 pages3.2. ECMO Cannulation and PitfallEko SarwowibowoPas encore d'évaluation
- Small Incision Cataract SurgeryDocument8 pagesSmall Incision Cataract Surgerykefi998100% (3)
- Temporal Bone Dissection ManualDocument15 pagesTemporal Bone Dissection Manualabhi2537100% (1)
- The Seldinger Technique-1Document26 pagesThe Seldinger Technique-1sanyengerePas encore d'évaluation
- Cornea WordDocument59 pagesCornea WordSana ParveenPas encore d'évaluation
- Harvesting SVGDocument26 pagesHarvesting SVGSamuel Hotma Rotua Sinaga100% (1)
- Steps Cataract ExtractionDocument9 pagesSteps Cataract ExtractionJustin John NavarroPas encore d'évaluation
- Management Eye Lid Laceration Pit FinalDocument30 pagesManagement Eye Lid Laceration Pit FinalLingula AurikulaPas encore d'évaluation
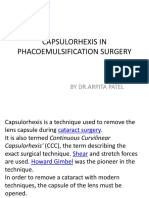
- Capsulorhexis in Phacoemulsification SurgeryDocument24 pagesCapsulorhexis in Phacoemulsification SurgeryPawan JarwalPas encore d'évaluation
- Nipple Reconstruction FINALDocument39 pagesNipple Reconstruction FINALBarath Kumar SinghPas encore d'évaluation
- Toric Iol: Dr. Ankit GuptaDocument28 pagesToric Iol: Dr. Ankit GuptaArif MohammadPas encore d'évaluation
- Eye and Ocular AdnexaDocument19 pagesEye and Ocular AdnexaANJALI RAWATPas encore d'évaluation
- Endoscopy Layth Mahmoud HussainDocument15 pagesEndoscopy Layth Mahmoud Hussainnoor deenPas encore d'évaluation
- Rhinoplasty 이홍경Document53 pagesRhinoplasty 이홍경entgo8282Pas encore d'évaluation
- Lens Anterior Capsule Opening ProceduresDocument15 pagesLens Anterior Capsule Opening ProceduresDr Sudhir SinghPas encore d'évaluation
- Cataract Coach BookDocument62 pagesCataract Coach Bookravian8bPas encore d'évaluation
- 07 Special E (Fako)Document21 pages07 Special E (Fako)srihandayaniakbarPas encore d'évaluation
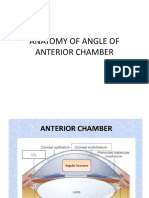
- Anatomy of Angle of Anterior ChamberDocument67 pagesAnatomy of Angle of Anterior ChamberRahnaPas encore d'évaluation
- Aqueous Drainage Devices: Major ReviewDocument3 pagesAqueous Drainage Devices: Major ReviewAhmad Angga LuthfiPas encore d'évaluation
- Dokumen - Tips RirsDocument98 pagesDokumen - Tips RirsBela RonaldoePas encore d'évaluation
- Extracapsular Cataract Extraction (Ecce)Document9 pagesExtracapsular Cataract Extraction (Ecce)Nica Lopez FernandezPas encore d'évaluation
- 05 EcceDocument9 pages05 EccebebibebihoPas encore d'évaluation
- Cataract And Small Pupil Management Manual Techniques: 2022, #1D'EverandCataract And Small Pupil Management Manual Techniques: 2022, #1Pas encore d'évaluation
- Trocar Surgery for Cataract Surgeons: From Dislocated IOL to Dropped NucleusD'EverandTrocar Surgery for Cataract Surgeons: From Dislocated IOL to Dropped NucleusPas encore d'évaluation
- Michelle L. Smith: Curriculum VitaeDocument5 pagesMichelle L. Smith: Curriculum Vitaeapi-327120894Pas encore d'évaluation
- Ed GeinDocument4 pagesEd GeinDaniel OxendinePas encore d'évaluation
- Genetic DisordersDocument26 pagesGenetic DisordersArresha100% (3)
- Act For Insomnia Act I by DR Guy Meadows The Sleep SchoolDocument7 pagesAct For Insomnia Act I by DR Guy Meadows The Sleep SchoolDharmendra KumarPas encore d'évaluation
- Hypertension CASE STUDYDocument30 pagesHypertension CASE STUDYKaloy Kamao100% (7)
- Constraints in Herbal MedicineDocument4 pagesConstraints in Herbal MedicinesebburgPas encore d'évaluation
- EnglishDocument16 pagesEnglishEugenius Divine LovePas encore d'évaluation
- Dispelling Myths About Drinking Distilled WaterDocument6 pagesDispelling Myths About Drinking Distilled WaterPau StraitPas encore d'évaluation
- Journal of Infection and Chemotherapy: Original ArticleDocument7 pagesJournal of Infection and Chemotherapy: Original ArticleNoNWOPas encore d'évaluation
- Marcapasos Cardiaco Externo ST Jude Medical 3077 SpecsDocument2 pagesMarcapasos Cardiaco Externo ST Jude Medical 3077 SpecsJair Jesús Cazares Rojas100% (1)
- Updates in The Treatment of Eating Disorders in 2022 A Year in Review in Eating Disorders The Journal of Treatment PreventionDocument12 pagesUpdates in The Treatment of Eating Disorders in 2022 A Year in Review in Eating Disorders The Journal of Treatment PreventionMarietta_MonariPas encore d'évaluation
- NEJMPsilocybinDocument12 pagesNEJMPsilocybinpaul casillasPas encore d'évaluation
- Clinical Pharmacology For LUSUMA NotesDocument110 pagesClinical Pharmacology For LUSUMA NotesTausif Huq100% (1)
- ASEA Athletics VT StudyDocument5 pagesASEA Athletics VT Studyalien asterixPas encore d'évaluation
- Banning BarbieDocument5 pagesBanning Barbieapi-267623773Pas encore d'évaluation
- Katerina P Reilly ResumeDocument2 pagesKaterina P Reilly Resumeapi-286221742Pas encore d'évaluation
- Chapter 70-GuytonDocument9 pagesChapter 70-Guytonswoljaswol1Pas encore d'évaluation
- Stress Burnout - Georgeann RoudebushDocument45 pagesStress Burnout - Georgeann RoudebushVinnyYusrainiPas encore d'évaluation
- Patient CounsellingDocument19 pagesPatient CounsellingchivconPas encore d'évaluation
- Pasifik Medikal CatalogueDocument24 pagesPasifik Medikal CatalogueAr ZahPas encore d'évaluation
- Health Drink - MKTDocument46 pagesHealth Drink - MKTGunjan BhattPas encore d'évaluation
- CBE - Platelet AbnormalitiesDocument3 pagesCBE - Platelet AbnormalitiesRuxandra MesarosPas encore d'évaluation
- DR Mahdavi - Mechanical VentilationDocument28 pagesDR Mahdavi - Mechanical VentilationHimanshu ShrimaliPas encore d'évaluation
- Partial MastectomyDocument17 pagesPartial MastectomyJill Rae Lloren ConsolacionPas encore d'évaluation
- Cerebral EdemaDocument15 pagesCerebral EdemaMae FlagerPas encore d'évaluation
- Dentine HypersensitivityDocument32 pagesDentine Hypersensitivityitdoc100% (1)
- Group Activities - Expressive TherapistDocument11 pagesGroup Activities - Expressive TherapistAlexandra Stancu100% (2)
- Drug Study RMCDocument3 pagesDrug Study RMCNicolo Paulo TabiraraPas encore d'évaluation
- Freud - Fetishism (1927e)Document6 pagesFreud - Fetishism (1927e)I Smith100% (1)
- ClexaneDocument2 pagesClexaneianecunar100% (2)