Vous aimerez peut-être aussi
- Diabeticum Ketoacidosis: Ach. Najich RF, DRDocument16 pagesDiabeticum Ketoacidosis: Ach. Najich RF, DRAch Najich RfPas encore d'évaluation
- Laporan Kasus KADDocument43 pagesLaporan Kasus KADharasthaPas encore d'évaluation
- RENAL EMERGENCIESDocument36 pagesRENAL EMERGENCIESPriscilla Christina NatanPas encore d'évaluation
- k20 - Stroke IskemikDocument35 pagesk20 - Stroke IskemikZikri Putra Lan LubisPas encore d'évaluation
- Acute Coronary Syndrome 052014Document91 pagesAcute Coronary Syndrome 052014Fatahillah NazarPas encore d'évaluation
- CHF LapsusDocument27 pagesCHF Lapsuseno46Pas encore d'évaluation
- Krisis Tiroid FixDocument38 pagesKrisis Tiroid FixVita DesriantiPas encore d'évaluation
- EKG PJK Co AssDocument115 pagesEKG PJK Co AsssalmaPas encore d'évaluation
- IPDIDocument30 pagesIPDIaris budionoPas encore d'évaluation
- Pembekalan PediatriDocument70 pagesPembekalan PediatrimilaimoetPas encore d'évaluation
- Acs TrombolitikDocument55 pagesAcs TrombolitikDiana IswardhaniPas encore d'évaluation
- Pediatri Essensial 3Document86 pagesPediatri Essensial 3Gregorius WahyudiPas encore d'évaluation
- Uremic LungDocument26 pagesUremic LungCitra Wulandari SofyanPas encore d'évaluation
- Regulasi Aliran Darah Cerebral Dan Aneurisma CerebralDocument12 pagesRegulasi Aliran Darah Cerebral Dan Aneurisma CerebralchandradwtrPas encore d'évaluation
- Types of Shock and Their ManagementDocument30 pagesTypes of Shock and Their ManagementPradnya PrabestiPas encore d'évaluation
- Catatan NeuroDocument36 pagesCatatan NeuroarinasanoPas encore d'évaluation
- Tata Laksana Sindroma Koroner Akut: Cholid Tri TjahjonoDocument84 pagesTata Laksana Sindroma Koroner Akut: Cholid Tri TjahjonoVio Alveolita PrimayaniPas encore d'évaluation
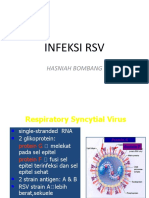
- Infeksi RSV: Hasniah BombangDocument12 pagesInfeksi RSV: Hasniah Bombangmuh hardiansyahPas encore d'évaluation
- Daftar Kode Diagnosa & TindakanDocument7 pagesDaftar Kode Diagnosa & Tindakannovi andriyaniPas encore d'évaluation
- Pembahasan CBT COMBO 3Document802 pagesPembahasan CBT COMBO 3Sari Dewi WiratsihPas encore d'évaluation
- Hypertension Treatment and GoalsDocument41 pagesHypertension Treatment and GoalsSemestaPas encore d'évaluation
- Monitoring OF Hemorrhagic Shock: Basrul HanafiDocument24 pagesMonitoring OF Hemorrhagic Shock: Basrul HanafiabdurrahmanPas encore d'évaluation
- Head Trauma Chapter 6Document43 pagesHead Trauma Chapter 6Aray Al-AfiqahPas encore d'évaluation
- CHF FC III Ec Mitral StenosisDocument36 pagesCHF FC III Ec Mitral Stenosisbroken18bear100% (1)
- Catatan Hitam PediatricDocument193 pagesCatatan Hitam Pediatricardhom122Pas encore d'évaluation
- Polycythemia Vera: Nurmaratu Thahirah Suaib C014172174Document12 pagesPolycythemia Vera: Nurmaratu Thahirah Suaib C014172174amiraPas encore d'évaluation
- Typhoid Fever Case ReportDocument32 pagesTyphoid Fever Case ReportAlvin PratamaPas encore d'évaluation
- Unlock-Forensik Etik Medikolegal - PESERTADocument156 pagesUnlock-Forensik Etik Medikolegal - PESERTAAde fathPas encore d'évaluation
- Lutembacher's Syndrome at KolonodaleDocument7 pagesLutembacher's Syndrome at KolonodaleWayan GunawanPas encore d'évaluation
- Gagal Napas: Pembimbing Dr. Ngakan Putu Parsama Putra, SPP (K) Presenter Dr. Muli YamanDocument20 pagesGagal Napas: Pembimbing Dr. Ngakan Putu Parsama Putra, SPP (K) Presenter Dr. Muli YamanAdlan BinharyantoPas encore d'évaluation
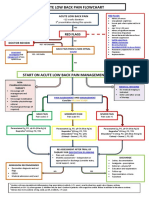
- Acute Low Back Pain Flowchart January 2017Document1 pageAcute Low Back Pain Flowchart January 20171234chocoPas encore d'évaluation
- Predicting the Etiology of CLABSI: Bacterial vs Fungal InfectionsDocument19 pagesPredicting the Etiology of CLABSI: Bacterial vs Fungal InfectionssilviPas encore d'évaluation
- Syok Kardiogenik PPT (3440) - 1Document18 pagesSyok Kardiogenik PPT (3440) - 1Mark YangPas encore d'évaluation
- Case Report EpistaksisDocument25 pagesCase Report EpistaksisarinasmithPas encore d'évaluation
- Fluid Management: Suparto Anesthesia Department Medical Faculty Christian Krida Wacana UniversityDocument61 pagesFluid Management: Suparto Anesthesia Department Medical Faculty Christian Krida Wacana UniversitygozaPas encore d'évaluation
- Sindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Document68 pagesSindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Dafhina Store100% (1)
- What Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)Document39 pagesWhat Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)laurentiaPas encore d'évaluation
- Trauma MataDocument57 pagesTrauma MataFatmala Umi MaisarahPas encore d'évaluation
- MANAGEMENT ACUTE ISCHEMIC STROKE (Simpo rTPA RSHS) - LisdaDocument63 pagesMANAGEMENT ACUTE ISCHEMIC STROKE (Simpo rTPA RSHS) - LisdadianPas encore d'évaluation
- ATLS FatmawatiDocument35 pagesATLS FatmawatiAnindya Anjas PutriaviPas encore d'évaluation
- Double Lumen Catheter Procedures and ComplicationsDocument20 pagesDouble Lumen Catheter Procedures and ComplicationsastarimediantoPas encore d'évaluation
- Kegawatdaruratan Pada Anak Dan Bayi: Kepaniteraan Klinik Emergensi RSUP Fatmawati Jakarta FKIK UIN Syarif HidayatullahDocument81 pagesKegawatdaruratan Pada Anak Dan Bayi: Kepaniteraan Klinik Emergensi RSUP Fatmawati Jakarta FKIK UIN Syarif HidayatullahJavar SodicPas encore d'évaluation
- PAD vs. DVTDocument3 pagesPAD vs. DVTKrystel BatinoPas encore d'évaluation
- Management Terapi Cairan Dr. AW 01Document60 pagesManagement Terapi Cairan Dr. AW 01Umhy GumianaPas encore d'évaluation
- Anaesthesia SummaryDocument36 pagesAnaesthesia SummaryRazan QassemPas encore d'évaluation
- Gagal Ginjal Akut Dan Kronik: Divisi Ginjal & Hipertensi SMF/Lab - Ilmu Penyakit Dalam FK - UNS / RSUD DR - MoewardiDocument29 pagesGagal Ginjal Akut Dan Kronik: Divisi Ginjal & Hipertensi SMF/Lab - Ilmu Penyakit Dalam FK - UNS / RSUD DR - MoewardiHabiby Habibaty QolbiPas encore d'évaluation
- Sistem Saraf dan Sistem GastrointestinalDocument8 pagesSistem Saraf dan Sistem GastrointestinalJosa Anggi PratamaPas encore d'évaluation
- Ketoasidosis DiabetikumDocument13 pagesKetoasidosis DiabetikumAdindapauliaPas encore d'évaluation
- Fluid TherapyDocument56 pagesFluid TherapyHabibie El RamadhaniPas encore d'évaluation
- Schematic Diagram: Predisposing PrecipitatingDocument5 pagesSchematic Diagram: Predisposing PrecipitatingKarl Wesley DillozonPas encore d'évaluation
- 2010 Integrated Updated Circulation ACLS Tachycardia AlgorithmDocument1 page2010 Integrated Updated Circulation ACLS Tachycardia AlgorithmRyggie ComelonPas encore d'évaluation
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- FK Uh, Rsup Ws. SPM Neurologi. Makassar. FK Uh, Rsup Ws. 2011Document80 pagesFK Uh, Rsup Ws. SPM Neurologi. Makassar. FK Uh, Rsup Ws. 2011Ryan TrianPas encore d'évaluation
- Craniosynostosis diagnosis and treatmentDocument12 pagesCraniosynostosis diagnosis and treatmentWaeel HamoudaPas encore d'évaluation
- (PESERTA) PEDIATRI 2 - MANTAP Februari 2017 PDFDocument157 pages(PESERTA) PEDIATRI 2 - MANTAP Februari 2017 PDFmarcelinaPas encore d'évaluation
- Askep MCI - AchirmanDocument53 pagesAskep MCI - AchirmanmarthaPas encore d'évaluation
- SCAI Shock Classification DeckDocument22 pagesSCAI Shock Classification DeckJimmy JimmyPas encore d'évaluation
- Hipertensi-Krisis Dr. HendroDocument35 pagesHipertensi-Krisis Dr. Hendroyudhagp100% (1)
- Diabetic Emergencies Case StudiesDocument32 pagesDiabetic Emergencies Case StudiesLamria Maloni Siahaan0% (1)
- DKAPPTxDocument34 pagesDKAPPTxMuhammad FurqanPas encore d'évaluation
- Ominous Octet For PharmacistsDocument16 pagesOminous Octet For PharmaciststreeshadowPas encore d'évaluation
- Daftar PustakaDocument6 pagesDaftar PustakaNur AzizahPas encore d'évaluation
- Adiposity 101.Document124 pagesAdiposity 101.Dr. Heath MotleyPas encore d'évaluation
- Jurnal Kad Dan HonkDocument9 pagesJurnal Kad Dan Honksimpati91Pas encore d'évaluation
- Shermeen Khan Contact 00923125142366: Introduction To Summaries of Chapters and Other Contents Sub Headings: Chapter OneDocument30 pagesShermeen Khan Contact 00923125142366: Introduction To Summaries of Chapters and Other Contents Sub Headings: Chapter Oneayeshaacademicuk20Pas encore d'évaluation
- Mhy Nuts Are Good FoodDocument1 pageMhy Nuts Are Good FoodSyazwan SaidanPas encore d'évaluation
- A Case of Haemochromatosis and Diabetes A Missed OpportunityDocument111 pagesA Case of Haemochromatosis and Diabetes A Missed Opportunitymimran1974Pas encore d'évaluation
- Overview of ForxigaDocument37 pagesOverview of ForxigaoctatransferPas encore d'évaluation
- Erasmus Medical Center NetherlandsDocument37 pagesErasmus Medical Center NetherlandsMarti MastersPas encore d'évaluation
- Diabetes MellitusDocument13 pagesDiabetes Mellitusdreneavalentinstefan100% (1)
- Beta-Cell-Mimetic Designer Cells Provide Closed-Loop Glycemic ControlDocument7 pagesBeta-Cell-Mimetic Designer Cells Provide Closed-Loop Glycemic ControlNando93Pas encore d'évaluation
- 1 Lose Weight at 50 and BeyondDocument16 pages1 Lose Weight at 50 and BeyondNebojsaPas encore d'évaluation
- Bab Ii Fix 6Document15 pagesBab Ii Fix 6Mellan Apriiaty SimbolonPas encore d'évaluation
- Trazodone Hydrochloride Side Effects - From FDA Reports - EHealthMeDocument3 pagesTrazodone Hydrochloride Side Effects - From FDA Reports - EHealthMelaniPas encore d'évaluation
- Irbesartan (Avapro)Document1 pageIrbesartan (Avapro)EPas encore d'évaluation
- EmpagliflozinDocument2 pagesEmpagliflozinAusaf AhmadPas encore d'évaluation
- Lowering - Glucose - Paragis For PRINTDocument25 pagesLowering - Glucose - Paragis For PRINTEUGENIO RIVERAPas encore d'évaluation
- Research Paper About ObesityDocument9 pagesResearch Paper About ObesityProsperoProllamante100% (1)
- 9 Benefits of Coenzyme Q10Document8 pages9 Benefits of Coenzyme Q10Anirban ChakrabortyPas encore d'évaluation
- Diet ManualDocument89 pagesDiet ManualPrema Bahadur0% (1)
- Jurnal DM Type 2 PDFDocument16 pagesJurnal DM Type 2 PDFAbd RahmanPas encore d'évaluation
- Balotario 1 Parcial Inles Tecnico 2Document4 pagesBalotario 1 Parcial Inles Tecnico 2JesúsChamorroPas encore d'évaluation
- Products Anti Diabetes For Type 1 and Type 2 Diabetes Natto Roots Momordica Balsamina Caju Bark Artemisia Afra TinctureDocument5 pagesProducts Anti Diabetes For Type 1 and Type 2 Diabetes Natto Roots Momordica Balsamina Caju Bark Artemisia Afra TinctureNile Valley MedicinePas encore d'évaluation
- Morning Report Physician In Charge Patients Summary Lab ResultsDocument23 pagesMorning Report Physician In Charge Patients Summary Lab ResultsMuhammad Bilal SaifulhaqPas encore d'évaluation
- Carbohydrate Addiction - North & South MagazineDocument5 pagesCarbohydrate Addiction - North & South MagazineAdrian HylandPas encore d'évaluation
- Hypoglycemia - 2014 Morales N DoronDocument8 pagesHypoglycemia - 2014 Morales N DoronDian Eka RamadhaniPas encore d'évaluation
- MZ 14Document68 pagesMZ 14Robert AndrejašPas encore d'évaluation
- Alcohol Benefits . Is Alcohol A Nutrient?Document45 pagesAlcohol Benefits . Is Alcohol A Nutrient?Malik Rizwan ElahiPas encore d'évaluation
- Endocrine Pancreas PharmacologyDocument38 pagesEndocrine Pancreas PharmacologydarkmagicdrakePas encore d'évaluation
- Diabetes Mellitus Insights Perspectives I To 13Document345 pagesDiabetes Mellitus Insights Perspectives I To 13tio_bsPas encore d'évaluation