Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- String Harmonics in Ravel's Orchestral WorksDocument97 pagesString Harmonics in Ravel's Orchestral WorksYork R83% (6)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- PZO9401 Second Darkness Players Guide PDFDocument36 pagesPZO9401 Second Darkness Players Guide PDFAllan ChuaPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Garcia vs. J. Drilon G. R. No. 179267 Case DigestDocument5 pagesGarcia vs. J. Drilon G. R. No. 179267 Case DigestJoannMarieBrenda delaGentePas encore d'évaluation
- Physics Project On Circular MotionDocument22 pagesPhysics Project On Circular Motionishan67% (3)
- Shaft Deflection in Centrifugal PumpsDocument2 pagesShaft Deflection in Centrifugal PumpsPieter van der WaltPas encore d'évaluation
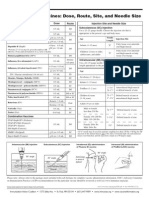
- Dosis Vaksin Anak AnakDocument1 pageDosis Vaksin Anak AnakRudolf Fernando WibowoPas encore d'évaluation
- Diltiazem Reduces Stroke Risk by 20% in NORDIL StudyDocument11 pagesDiltiazem Reduces Stroke Risk by 20% in NORDIL StudyRudolf Fernando WibowoPas encore d'évaluation
- Induction of Labor and Risk of Postpartum Hemorrhage in Low Risk ParturientsDocument8 pagesInduction of Labor and Risk of Postpartum Hemorrhage in Low Risk ParturientsRudolf Fernando WibowoPas encore d'évaluation
- AsdbasjhfbswhefbehgvjhsvfdndbfnsbdfnebwnmfbenfmebmfefefefefeadwedwqdbkbfejkbfkbfwekjbfewjkfbewjkbfwejkystemDocument63 pagesAsdbasjhfbswhefbehgvjhsvfdndbfnsbdfnebwnmfbenfmebmfefefefefeadwedwqdbkbfejkbfkbfwekjbfewjkfbewjkbfwejkystemRudolf Fernando WibowoPas encore d'évaluation
- Carotid Cavernous Fistula: Images in Clinical MedicineDocument1 pageCarotid Cavernous Fistula: Images in Clinical MedicineRudolf Fernando WibowoPas encore d'évaluation
- Hepatitis Akut: Tinjauan PustakaDocument26 pagesHepatitis Akut: Tinjauan PustakaRudolf Fernando WibowoPas encore d'évaluation
- HPV in Progress PterygiumDocument3 pagesHPV in Progress PterygiumRudolf Fernando WibowoPas encore d'évaluation
- What Is The Value of Incorporating Tear Osmolarity Measurement in Assessing Patient Response To Therapy in Dry Eye DiseaseDocument11 pagesWhat Is The Value of Incorporating Tear Osmolarity Measurement in Assessing Patient Response To Therapy in Dry Eye DiseaseRudolf Fernando WibowoPas encore d'évaluation
- Retinal Detachment after Open Globe Injury Risk FactorsDocument7 pagesRetinal Detachment after Open Globe Injury Risk FactorsRudolf Fernando WibowoPas encore d'évaluation
- HPV in Progress PterygiumDocument3 pagesHPV in Progress PterygiumRudolf Fernando WibowoPas encore d'évaluation
- Cataract Surgery in Glaucoma Patients How Much BenefitDocument3 pagesCataract Surgery in Glaucoma Patients How Much BenefitRudolf Fernando WibowoPas encore d'évaluation
- AcanthamoebaDocument7 pagesAcanthamoebaYohanna YohannaPas encore d'évaluation
- New BMI Criteria for Screening Metabolic SyndromeDocument9 pagesNew BMI Criteria for Screening Metabolic SyndromeRudolf Fernando WibowoPas encore d'évaluation
- New BMI Criteria for Screening Metabolic SyndromeDocument9 pagesNew BMI Criteria for Screening Metabolic SyndromeRudolf Fernando WibowoPas encore d'évaluation
- Theresia Veronika 405100017: Pemicu 3A UrogenitalDocument87 pagesTheresia Veronika 405100017: Pemicu 3A UrogenitalRudolf Fernando WibowoPas encore d'évaluation
- Explain Mod 4Document20 pagesExplain Mod 4Gab IgnacioPas encore d'évaluation
- 1.MIL 1. Introduction To MIL Part 2 Characteristics of Information Literate Individual and Importance of MILDocument24 pages1.MIL 1. Introduction To MIL Part 2 Characteristics of Information Literate Individual and Importance of MILBernadette MendozaPas encore d'évaluation
- Contract Costing - Practise ProblemsDocument3 pagesContract Costing - Practise ProblemsMadhavasadasivan Pothiyil50% (2)
- Edgar Allan Poe's "The RavenDocument3 pagesEdgar Allan Poe's "The RavenЖанна ФодееваPas encore d'évaluation
- Depository Receipts: Presented By-Vikash Sharma (51) Ruchi BangaDocument12 pagesDepository Receipts: Presented By-Vikash Sharma (51) Ruchi Bangasuraj kumar0% (1)
- ''Let All God's Angels Worship Him'' - Gordon AllanDocument8 pages''Let All God's Angels Worship Him'' - Gordon AllanRubem_CLPas encore d'évaluation
- Research Scholar Progress Report Review FormDocument3 pagesResearch Scholar Progress Report Review FormYepuru ChaithanyaPas encore d'évaluation
- Volleyball TermsDocument2 pagesVolleyball TermskimmybapkiddingPas encore d'évaluation
- 일반동사 부정문 PDFDocument5 pages일반동사 부정문 PDF엄태호Pas encore d'évaluation
- French demonstrative pronouns guideDocument8 pagesFrench demonstrative pronouns guidedfñoiiuglkjs.Pas encore d'évaluation
- Song Grade XiDocument12 pagesSong Grade XiM Ridho KurniawanPas encore d'évaluation
- Conquest of The Americas (Eakin-2002)Document81 pagesConquest of The Americas (Eakin-2002)GregPas encore d'évaluation
- Shamanhood and Mythology: Archaic Techniques of Ecstasy and Current Techniques of ResearchDocument22 pagesShamanhood and Mythology: Archaic Techniques of Ecstasy and Current Techniques of ResearchDunja Chrysina ChrysargyreaPas encore d'évaluation
- Allosteric EnzymeDocument22 pagesAllosteric EnzymeAhmed ImranPas encore d'évaluation
- Director VP Program Manager in Raleigh NC Resume Mary Paige ForresterDocument6 pagesDirector VP Program Manager in Raleigh NC Resume Mary Paige ForresterMaryPaigeForresterPas encore d'évaluation
- Eq 1Document4 pagesEq 1jppblckmnPas encore d'évaluation
- GEY 102-Introduction To Geology 1-Lecture Slides - Prof. M.E. NtonDocument44 pagesGEY 102-Introduction To Geology 1-Lecture Slides - Prof. M.E. Ntonabuabdmuqseet2001Pas encore d'évaluation
- TEACHING AS A NOBLE PROFESSIONDocument6 pagesTEACHING AS A NOBLE PROFESSIONShaiPas encore d'évaluation
- Exery Analysis of Vapour Compression Refrigeration SystemDocument22 pagesExery Analysis of Vapour Compression Refrigeration Systemthprasads8356Pas encore d'évaluation
- New Dll-Math Week 4-1Document3 pagesNew Dll-Math Week 4-1AstroPas encore d'évaluation
- Métodos de Reabilitação para Redução Da Subluxação Do Ombro Na Hemiparesia pós-AVC Uma Revisão SistemátDocument15 pagesMétodos de Reabilitação para Redução Da Subluxação Do Ombro Na Hemiparesia pós-AVC Uma Revisão SistemátMatheus AlmeidaPas encore d'évaluation
- Coursework of Signals and Systems: Moh. Kamalul Wafi December 6, 2018Document2 pagesCoursework of Signals and Systems: Moh. Kamalul Wafi December 6, 2018kartiniPas encore d'évaluation
- Paradine V Jane - (1646) 82 ER 897Document2 pagesParadine V Jane - (1646) 82 ER 897TimishaPas encore d'évaluation
- Impact of Technology On Future JobsDocument29 pagesImpact of Technology On Future Jobsmehrunnisa99Pas encore d'évaluation