Vous aimerez peut-être aussi
- Ten Metacognitive Teaching StrategiesDocument20 pagesTen Metacognitive Teaching StrategiesMark Joseph Nepomuceno Cometa100% (2)
- Session Guide: Session Tittle Session ObjectivesDocument3 pagesSession Guide: Session Tittle Session ObjectivesMahir Bualan Amba100% (4)
- Individual Performance Commitment and Review Form (Ipcrf) For TeachersDocument6 pagesIndividual Performance Commitment and Review Form (Ipcrf) For TeachersNoel Grey50% (4)
- Introduction To Greek DramaDocument26 pagesIntroduction To Greek DramaGael Forbes Real100% (1)
- GUIDELINES FOR ADMINISTERING DIVISION QUARTERLY TESTSDocument10 pagesGUIDELINES FOR ADMINISTERING DIVISION QUARTERLY TESTSJhun MarkPas encore d'évaluation
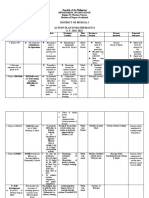
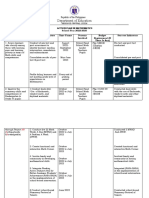
- District of Murcia 1 Action Plan in Mathematics S. Y. 2021-2022Document4 pagesDistrict of Murcia 1 Action Plan in Mathematics S. Y. 2021-2022Dore EstampaPas encore d'évaluation
- Basic Education Exit Assessment Beea For Grade 12 2019Document53 pagesBasic Education Exit Assessment Beea For Grade 12 2019Cjay Maningas75% (12)
- Department of Education: Republic of The Philippines Region Iv-A Calabarzon Division of Rizal District of Binangonan IIIDocument1 pageDepartment of Education: Republic of The Philippines Region Iv-A Calabarzon Division of Rizal District of Binangonan IIIArenas Jen100% (1)
- SUPERVISORY PLAN For MTsDocument7 pagesSUPERVISORY PLAN For MTsgerome negad100% (1)
- Grade 7 Science Motion GuideDocument16 pagesGrade 7 Science Motion GuideGael Forbes Real78% (9)
- Grade 6 DLL ENGLISH 6 Q3 Week 3Document3 pagesGrade 6 DLL ENGLISH 6 Q3 Week 3Gaelle CBPas encore d'évaluation
- Working Committee For Early RegistrationDocument4 pagesWorking Committee For Early RegistrationKent DaradarPas encore d'évaluation
- College Readiness of Senior High School StudentsDocument10 pagesCollege Readiness of Senior High School StudentsBea C. Masujer83% (6)
- Erroneously TaggedDocument1 pageErroneously TaggedDivina Veloso Aman0% (1)
- Session Guide On (Egma) - Early Grade Mathematics AssessmentDocument2 pagesSession Guide On (Egma) - Early Grade Mathematics AssessmentKenshin Himura Perez50% (2)
- Early Grade Mathematics Assessment Grade 1 (ORAL TEST - Teachers' Copy)Document12 pagesEarly Grade Mathematics Assessment Grade 1 (ORAL TEST - Teachers' Copy)Riza Guste100% (1)
- 7 Pasidungog Search: Annex ADocument4 pages7 Pasidungog Search: Annex AAllanSalardaAdem100% (1)
- SMAW Welding Training GuideDocument123 pagesSMAW Welding Training Guidevictor100% (2)
- Levelling of ExpectationsDocument5 pagesLevelling of Expectationschepie creenciaPas encore d'évaluation
- Accomplishment ReportDocument1 pageAccomplishment ReportJESSA SUMAYANGPas encore d'évaluation
- Selection Guidelines On The NAT G10 AllocationDocument33 pagesSelection Guidelines On The NAT G10 AllocationCatherine Libuna100% (2)
- Quarter 2 Math 6 Week 5Document19 pagesQuarter 2 Math 6 Week 5Quenie LustadoPas encore d'évaluation
- eSAT 2019Document6 pageseSAT 2019venus velonza100% (2)
- Elvina B. Canipas Ipcrf 2015 2016Document21 pagesElvina B. Canipas Ipcrf 2015 2016LeonorBagnison67% (3)
- Activity Completion Report - MtapDocument17 pagesActivity Completion Report - MtapLourd Edmond Carlisle DantesPas encore d'évaluation
- Accomplishment Report IN MathematicsDocument4 pagesAccomplishment Report IN MathematicsMark Kiven Martinez100% (1)
- R6 G1 BoSY CRLA Scoresheet - v6 - (Teachername - Schoolname)Document14 pagesR6 G1 BoSY CRLA Scoresheet - v6 - (Teachername - Schoolname)Mar Stone100% (3)
- Learning Recovery Continuity Plan in NumeracyDocument3 pagesLearning Recovery Continuity Plan in NumeracyMaia Alvarez100% (1)
- Training Matrix: 3RD School-Based Math CampDocument2 pagesTraining Matrix: 3RD School-Based Math CampEvelynPas encore d'évaluation
- LAC Implementation ProcessDocument20 pagesLAC Implementation ProcessShara Faye GalpaoPas encore d'évaluation
- SDO Bataan Elementary School Math Action Plan 2022-2023Document2 pagesSDO Bataan Elementary School Math Action Plan 2022-2023Archie Buenviaje Alarcon50% (2)
- Process Observation Tool ReviewDocument2 pagesProcess Observation Tool ReviewAroma Eyre100% (3)
- Narrative Report On Project Numbers (Numerals Use To Make Brain Exercise To Reinforce Non-Numerate Students)Document2 pagesNarrative Report On Project Numbers (Numerals Use To Make Brain Exercise To Reinforce Non-Numerate Students)Ako Para Sau100% (4)
- Lac Session For TeachersDocument1 pageLac Session For TeachersXer WinchesterPas encore d'évaluation
- OHSP HandbookDocument23 pagesOHSP HandbookJoel Puruganan SaladinoPas encore d'évaluation
- OHSP HandbookDocument23 pagesOHSP HandbookJoel Puruganan SaladinoPas encore d'évaluation
- Bea Form 1Document1 pageBea Form 1Keith Owen Garcia100% (3)
- 2014 Grade Six Consolidated Class ProgramDocument7 pages2014 Grade Six Consolidated Class ProgramcatherinerenantePas encore d'évaluation
- Project MathALINO Action PlanDocument3 pagesProject MathALINO Action PlanMaestro Varix100% (2)
- Cid Me Form 1a and Form 1bDocument5 pagesCid Me Form 1a and Form 1berosh100% (3)
- SP2ES Action Plan in Math 2022 2023Document4 pagesSP2ES Action Plan in Math 2022 2023Amiel Garcia100% (1)
- Molopolo National High School Lists Least Mastered Math CompetenciesDocument1 pageMolopolo National High School Lists Least Mastered Math CompetenciesGlaiza Asentista Mangaron Lazaga100% (1)
- Bilogo Elementary School: Child-Friendly School SurveyDocument49 pagesBilogo Elementary School: Child-Friendly School SurveyRosemarie AguilarPas encore d'évaluation
- Peer Observation and Feedback 2Document25 pagesPeer Observation and Feedback 2api-54711323Pas encore d'évaluation
- Instructional Supervision Monitoring Tool For Teachers: Areas' Highly Evident Evident Not Evident MovsDocument2 pagesInstructional Supervision Monitoring Tool For Teachers: Areas' Highly Evident Evident Not Evident MovsGael Forbes Real100% (5)
- Instructional Supervision Monitoring Tool For Teachers: Areas' Highly Evident Evident Not Evident MovsDocument2 pagesInstructional Supervision Monitoring Tool For Teachers: Areas' Highly Evident Evident Not Evident MovsGael Forbes Real100% (5)
- 2014 Nat Comprehension Check-Edited 1.7.14Document2 pages2014 Nat Comprehension Check-Edited 1.7.14Dhan Bunsoy100% (2)
- Early Language, Literacy, and Numeracy Assessment National Achievement Test For Grade 6Document30 pagesEarly Language, Literacy, and Numeracy Assessment National Achievement Test For Grade 6Ma Michelle FranciscoPas encore d'évaluation
- AGE LEVEL SPECIALIZATION COURSE - Baldovino, Angelu D. - OUTPUT - PRE-TASKDocument5 pagesAGE LEVEL SPECIALIZATION COURSE - Baldovino, Angelu D. - OUTPUT - PRE-TASKAngelu BaldovinoPas encore d'évaluation
- Appendix C 02 COT RPMS Rating Sheet For T I III For SY 2022 2023Document1 pageAppendix C 02 COT RPMS Rating Sheet For T I III For SY 2022 2023KEICHIE QUIMCO100% (5)
- School Memo For School Based Math FestivalDocument2 pagesSchool Memo For School Based Math FestivalRovie Saz100% (2)
- Republic of The Philippines Department of Education: Blasan Elementary SchoolDocument7 pagesRepublic of The Philippines Department of Education: Blasan Elementary SchoolArapoc Nikko DavePas encore d'évaluation
- Composition of Learning Action Cell S.Y. 2020-2021: Lac LeaderDocument1 pageComposition of Learning Action Cell S.Y. 2020-2021: Lac LeaderJen ApinadoPas encore d'évaluation
- Minutes of Management Committee MeetingDocument4 pagesMinutes of Management Committee Meetingcyrellejay mantalabaPas encore d'évaluation
- Action Plan in Mathematics PDF FreeDocument3 pagesAction Plan in Mathematics PDF FreeMary June DemontevwrdePas encore d'évaluation
- Mechanics of The Math Challenge 2020: (Grade 1 To 4) A. Final RoundDocument2 pagesMechanics of The Math Challenge 2020: (Grade 1 To 4) A. Final RoundAiv YlananPas encore d'évaluation
- Dupo Elementary School Parent Feedback FormDocument1 pageDupo Elementary School Parent Feedback FormSheryl SilangPas encore d'évaluation
- Star Scout Registration FormDocument1 pageStar Scout Registration Formmaestro24100% (1)
- Minutes On Focus Group DiscussionDocument3 pagesMinutes On Focus Group Discussionrico mol100% (1)
- Life is a Math equationDocument25 pagesLife is a Math equationGirlie Ann A MarquezPas encore d'évaluation
- Weekly Home Learning Plan for Visayan Village Central ElementaryDocument3 pagesWeekly Home Learning Plan for Visayan Village Central ElementaryCristy Amor Tedlos100% (1)
- VI-2 Phil-Iri-Filipino-Automated - 2019-2020Document48 pagesVI-2 Phil-Iri-Filipino-Automated - 2019-2020baldo yellow4Pas encore d'évaluation
- Rapid Mathematics AssessmentDocument68 pagesRapid Mathematics Assessmentjoemarie.dizon.personal100% (1)
- ACR in Conducting Numeracy TestDocument13 pagesACR in Conducting Numeracy TestMarissa Golong Silagan100% (1)
- Action Plan On Reading Remediation ProgramDocument3 pagesAction Plan On Reading Remediation ProgramJeffrey EstolePas encore d'évaluation
- Accomplishment Report MATH 2022-2023Document3 pagesAccomplishment Report MATH 2022-2023Donna Claire Villanueva-Evangelista100% (1)
- Inset Training Matrix Downloadable SampleDocument3 pagesInset Training Matrix Downloadable SampleMalou EvangelioPas encore d'évaluation
- Rufu Dela Cruz Intervention Plan Increases MasteryDocument6 pagesRufu Dela Cruz Intervention Plan Increases MasteryVENGIE PAMANPas encore d'évaluation
- BSP Parental ConsentDocument2 pagesBSP Parental ConsentJaymar S. VillarminoPas encore d'évaluation
- Department Of: Republic of The PhilippinesDocument9 pagesDepartment Of: Republic of The PhilippinesCebomailo Primary School Annex North CotabatoPas encore d'évaluation
- Republic of The PhilippinesDocument1 pageRepublic of The PhilippinesClaire CayangcangPas encore d'évaluation
- Before, During and After An Earthquake BeforeDocument2 pagesBefore, During and After An Earthquake BeforeGael Forbes RealPas encore d'évaluation
- ROY G. BIV on PaperDocument4 pagesROY G. BIV on PaperGael Forbes RealPas encore d'évaluation
- Blank NcbtsDocument86 pagesBlank NcbtsGael Forbes RealPas encore d'évaluation
- CBC-Beauty Care Services (Nail Care) NC IIDocument66 pagesCBC-Beauty Care Services (Nail Care) NC IIMc Suan100% (5)
- CBC-Beauty Care Services (Nail Care) NC IIDocument66 pagesCBC-Beauty Care Services (Nail Care) NC IIMc Suan100% (5)
- Science 7 Module 1Document14 pagesScience 7 Module 1Gael Forbes RealPas encore d'évaluation
- Countdown ClockDocument69 pagesCountdown ClockGael Forbes RealPas encore d'évaluation
- Grading Sheet K-12 For Sy 2015-2016 (Mapeh)Document47 pagesGrading Sheet K-12 For Sy 2015-2016 (Mapeh)Gael Forbes RealPas encore d'évaluation
- Educationalperiod 130705092455 Phpapp01Document11 pagesEducationalperiod 130705092455 Phpapp01Gael Forbes RealPas encore d'évaluation
- Memorandum 4770Document3 pagesMemorandum 4770Gael Forbes RealPas encore d'évaluation
- Instructional Supervision Handbook PDFDocument42 pagesInstructional Supervision Handbook PDFTonet Miralles88% (26)
- Manual For EmployeesDocument59 pagesManual For EmployeesGael Forbes RealPas encore d'évaluation
- Regional Memorandum No.13 s.2014Document2 pagesRegional Memorandum No.13 s.2014Gael Forbes RealPas encore d'évaluation
- The Non-Vascular to Vascular Plant KingdomDocument7 pagesThe Non-Vascular to Vascular Plant KingdomGael Forbes RealPas encore d'évaluation
- Music and Art - K To 12 Curriculum GuideDocument105 pagesMusic and Art - K To 12 Curriculum GuideFrancis A. Buenaventura33% (3)
- Or Molecular Structure Is The Three-Dimensional Arrangement of Atoms Within A MoleculeDocument38 pagesOr Molecular Structure Is The Three-Dimensional Arrangement of Atoms Within A MoleculeGael Forbes RealPas encore d'évaluation
- Deped Order No. 70 S. 2012Document3 pagesDeped Order No. 70 S. 2012bicchuchuPas encore d'évaluation
- Bios TatDocument12 pagesBios TatGael Forbes RealPas encore d'évaluation
- Clostridium Tetani: Scientific ClassificationDocument4 pagesClostridium Tetani: Scientific ClassificationGael Forbes RealPas encore d'évaluation
- HivDocument52 pagesHivGael Forbes RealPas encore d'évaluation
- Intro To College Student Guide 2019Document7 pagesIntro To College Student Guide 2019Muhammad AwaisPas encore d'évaluation
- Instructional Planning Guide on Demand and SupplyDocument3 pagesInstructional Planning Guide on Demand and SupplyRaffy Jade SalazarPas encore d'évaluation
- Soas Prospectus 2015Document248 pagesSoas Prospectus 2015Raies Ul-Haq Ahmad SikanderPas encore d'évaluation
- Choate Self-Assessment Predicts Student SuccessDocument5 pagesChoate Self-Assessment Predicts Student SuccessdbircsnPas encore d'évaluation
- Arts at The Core: Every School, Every StudentDocument36 pagesArts at The Core: Every School, Every StudentArts Alliance Illinois100% (1)
- LINUS2.0 English Literacy Programme ModulesDocument2 pagesLINUS2.0 English Literacy Programme ModulesZulaiha Abdul RahmanPas encore d'évaluation
- Venn Diagram Lesson Plan for Grade 10 MathDocument2 pagesVenn Diagram Lesson Plan for Grade 10 MathAljean TrinioPas encore d'évaluation
- A Private School Is Autonomous and Generates Its Own Funding Through Various Sources Like Student Tuition, Private Grants and EndowmentsDocument19 pagesA Private School Is Autonomous and Generates Its Own Funding Through Various Sources Like Student Tuition, Private Grants and EndowmentsRolyn ManansalaPas encore d'évaluation
- Bandura and Maslow HandoutDocument5 pagesBandura and Maslow Handoutapi-296978454Pas encore d'évaluation
- Causative VerbsDocument4 pagesCausative VerbsJE RelPas encore d'évaluation
- RazkidsDocument9 pagesRazkidsapi-434351600Pas encore d'évaluation
- Edward L. Thorndike, E O Bregman, M V Cobb, EllaDocument636 pagesEdward L. Thorndike, E O Bregman, M V Cobb, EllaCarlos LimonPas encore d'évaluation
- Minutes of The MeetingDocument3 pagesMinutes of The MeetinganirPas encore d'évaluation
- 2016 IAESTE OffersDocument2 pages2016 IAESTE OffersVirginia VirgiePas encore d'évaluation
- Book Extension Activity Lesson Plan Dragons Love TacosDocument2 pagesBook Extension Activity Lesson Plan Dragons Love Tacosapi-385165219Pas encore d'évaluation
- Rocket Review 4-29-14Document8 pagesRocket Review 4-29-14Theresa Parks StagerPas encore d'évaluation
- Please ReadDocument3 pagesPlease ReadSher SherwinPas encore d'évaluation
- Motivational Letter 27.07.20, Iasi Dear Sir / MadamDocument2 pagesMotivational Letter 27.07.20, Iasi Dear Sir / MadamAnaMariaPas encore d'évaluation
- Report 1Document4 pagesReport 1api-442426711Pas encore d'évaluation
- Abstract Faisal SajjadDocument1 pageAbstract Faisal SajjadMaria KhanPas encore d'évaluation
- Explore the 5 Senses Through Dialogue in the DarkDocument5 pagesExplore the 5 Senses Through Dialogue in the DarkhuntclubPas encore d'évaluation
- CBTS Fees Funding Info Booklet 2010 FinalDocument8 pagesCBTS Fees Funding Info Booklet 2010 FinalJoey LeePas encore d'évaluation
- Student Handbook 2016 FinalDocument22 pagesStudent Handbook 2016 FinalAquilia FranklinPas encore d'évaluation
- Bluefield State College Student HandbookDocument55 pagesBluefield State College Student HandbookbluefieldstatePas encore d'évaluation
- Communication Strategies in SLADocument3 pagesCommunication Strategies in SLAman_dainese100% (4)
- Challenges in ODLDocument21 pagesChallenges in ODLAhmad Shukri ZakariaPas encore d'évaluation