Vous aimerez peut-être aussi
- Portal Hypertension, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandPortal Hypertension, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsPas encore d'évaluation
- Tuberculous Meningitis: Manual of Diagnosis and TherapyD'EverandTuberculous Meningitis: Manual of Diagnosis and TherapyJerome ChinPas encore d'évaluation
- Congenital and Acquired Bone Marrow FailureD'EverandCongenital and Acquired Bone Marrow FailureMahmoud Deeb AljurfPas encore d'évaluation
- Problem-based Approach to Gastroenterology and HepatologyD'EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisPas encore d'évaluation
- ASCITESDocument25 pagesASCITESGanesh BabuPas encore d'évaluation
- Anesthesia for Congenital Heart DiseaseD'EverandAnesthesia for Congenital Heart DiseaseStephen A. StayerPas encore d'évaluation
- Pharmacology of Cardiac Function: Section of Pharmacology of the International Union of Physiological SciencesD'EverandPharmacology of Cardiac Function: Section of Pharmacology of the International Union of Physiological SciencesOtto KrayerPas encore d'évaluation
- Hiv-Associated Nephropathy (Hivan) : DR KibaruDocument27 pagesHiv-Associated Nephropathy (Hivan) : DR KibaruMalueth AnguiPas encore d'évaluation
- Infective Endocarditis: A Multidisciplinary ApproachD'EverandInfective Endocarditis: A Multidisciplinary ApproachArman KilicPas encore d'évaluation
- HivDocument36 pagesHivfenendriyaniPas encore d'évaluation
- Descending ParalysisDocument7 pagesDescending ParalysisgianpinotPas encore d'évaluation
- Pancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandPancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Approach To Abdominal Pain in The EdDocument88 pagesApproach To Abdominal Pain in The EdAmatul Billah AhmadPas encore d'évaluation
- Nephrotic Syndrome in Children: January 2013Document7 pagesNephrotic Syndrome in Children: January 2013molenPas encore d'évaluation
- Clinical Approach To RPRF PDFDocument6 pagesClinical Approach To RPRF PDFshankarPas encore d'évaluation
- Congenital Heart Diseases, A Simple Guide to these Medical ConditionsD'EverandCongenital Heart Diseases, A Simple Guide to these Medical ConditionsPas encore d'évaluation
- Tubulointerstitial Diseases: Dr. Raid JastaniaDocument48 pagesTubulointerstitial Diseases: Dr. Raid JastaniaThomas McconnellPas encore d'évaluation
- 2 PneumoniaDocument53 pages2 PneumoniaLucyellowOttemoesoePas encore d'évaluation
- Valvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMDocument69 pagesValvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMAbanoub AwadallaPas encore d'évaluation
- Henoch Schönlein PurpuraDocument12 pagesHenoch Schönlein PurpuraRavania Rahadian Putri100% (1)
- Renal Tubular AcidosisDocument32 pagesRenal Tubular AcidosisSimon OnsongoPas encore d'évaluation
- Management of Tuberculosis: A guide for clinicians (eBook edition)D'EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Pas encore d'évaluation
- Approach: A. How The Kidney Handle The Proteins?Document9 pagesApproach: A. How The Kidney Handle The Proteins?Rashed ShatnawiPas encore d'évaluation
- Left Ventricular Non-CompactionDocument20 pagesLeft Ventricular Non-CompactionlawlietPas encore d'évaluation
- Anak 3.1 Infective Endocarditis DRTLTDocument21 pagesAnak 3.1 Infective Endocarditis DRTLTAnastasia PinkyPas encore d'évaluation
- Bagian Patologi Anatomi Fk-Uisu 2011Document22 pagesBagian Patologi Anatomi Fk-Uisu 2011rizapuspairyaniPas encore d'évaluation
- Embryology and Development of KidneyDocument75 pagesEmbryology and Development of Kidneyranjitha sraatePas encore d'évaluation
- Practical Gastroenterology and Hepatology Board Review ToolkitD'EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultPas encore d'évaluation
- Pyrexia of Unknown OriginDocument81 pagesPyrexia of Unknown OriginJithin Bhagavati Kalam100% (1)
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsD'EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsPas encore d'évaluation
- Interventional Cardiology: Principles and PracticeD'EverandInterventional Cardiology: Principles and PracticeCarlo Di MarioPas encore d'évaluation
- VasculitidesDocument13 pagesVasculitidesIrene Zae MwandotoPas encore d'évaluation
- Ascites Hrs B WPDocument101 pagesAscites Hrs B WPGhias Un Nabi TayyabPas encore d'évaluation
- Infective Endocarditis: Ainal Fadly Adigama PF Enny SuryantiDocument50 pagesInfective Endocarditis: Ainal Fadly Adigama PF Enny SuryantiFaisal Reza AdiebPas encore d'évaluation
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Presented By: Dr. Hirdesh Chawla Junior Resident IiiDocument79 pagesPresented By: Dr. Hirdesh Chawla Junior Resident IiiAzizan HannyPas encore d'évaluation
- (Lecture) Approach To AscitesDocument48 pages(Lecture) Approach To AscitesJirayu Puthhai100% (1)
- Chronic Heart Failure ASHPDocument20 pagesChronic Heart Failure ASHPFaizan Mazhar100% (1)
- The Beta-Blocker Story: Getting It RightD'EverandThe Beta-Blocker Story: Getting It RightÉvaluation : 5 sur 5 étoiles5/5 (1)
- Spectrum of Acute Coronary Syndrome: Milagros Estrada-Yamamoto, MDDocument62 pagesSpectrum of Acute Coronary Syndrome: Milagros Estrada-Yamamoto, MDAnonymous HH3c17osPas encore d'évaluation
- Management of Diabetic Ketoacidosis in Children and AdolescentsDocument8 pagesManagement of Diabetic Ketoacidosis in Children and AdolescentsnurlatifahPas encore d'évaluation
- Jurnal PNHDocument10 pagesJurnal PNHsoriaputuPas encore d'évaluation
- Gastrointestinal Diseases and Disorders Sourcebook, Fifth EditionD'EverandGastrointestinal Diseases and Disorders Sourcebook, Fifth EditionPas encore d'évaluation
- Adenosine: Hillel Yaffe Medical CenterDocument1 pageAdenosine: Hillel Yaffe Medical CenteranaskabahaPas encore d'évaluation
- Forensic MedicineDocument113 pagesForensic Medicineanaskabaha100% (2)
- Forensic MedicineDocument113 pagesForensic Medicineanaskabaha100% (2)
- Multiple Myeloma and Related Disorders: Kumar RajagopalanDocument71 pagesMultiple Myeloma and Related Disorders: Kumar RajagopalananaskabahaPas encore d'évaluation
- Cardiology Board Review 2008 1215092899624216 8Document157 pagesCardiology Board Review 2008 1215092899624216 8anaskabaha100% (5)
- Mood DisordersDocument29 pagesMood DisordersanaskabahaPas encore d'évaluation
- CXR (2010 C1)Document103 pagesCXR (2010 C1)anaskabahaPas encore d'évaluation
- TOXO Presentation ENGLDocument20 pagesTOXO Presentation ENGLanaskabahaPas encore d'évaluation
- TOXO Presentation ENGLDocument20 pagesTOXO Presentation ENGLanaskabahaPas encore d'évaluation
- ObstetricsDocument46 pagesObstetricsanaskabaha100% (3)
- ECG InerpretitionDocument12 pagesECG InerpretitionMended_Heart100% (6)
- China Animal Healthcare: The Healing TouchDocument19 pagesChina Animal Healthcare: The Healing TouchBin WeiPas encore d'évaluation
- Test Container Form Lab Process Remarks HKL (Hospital Appointment Date - Specialist's SignatureDocument9 pagesTest Container Form Lab Process Remarks HKL (Hospital Appointment Date - Specialist's SignaturesyasyaPas encore d'évaluation
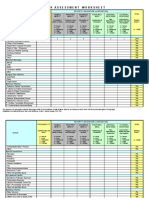
- IC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Document4 pagesIC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Juon Vairzya AnggraeniPas encore d'évaluation
- Egger & Angold, 2006 Disorders - DiscussionDocument25 pagesEgger & Angold, 2006 Disorders - DiscussionAlkistis MarinakiPas encore d'évaluation
- Tobacco Cessation PlanDocument11 pagesTobacco Cessation PlanEsteban García EcheverryPas encore d'évaluation
- Liver Meeting Brochure 2016 PDFDocument4 pagesLiver Meeting Brochure 2016 PDFManas GhoshPas encore d'évaluation
- Sri Lanka - Averting A National Nutrition Anomaly 2Document16 pagesSri Lanka - Averting A National Nutrition Anomaly 2Rushan LakdimuthuPas encore d'évaluation
- Bedwetting in ChildrenDocument41 pagesBedwetting in ChildrenAnkit ManglaPas encore d'évaluation
- Hypnosis For Irritable Bowel SyndromeDocument3 pagesHypnosis For Irritable Bowel SyndromeImam Abidin0% (1)
- Tes TLMDocument16 pagesTes TLMAmelia RosyidaPas encore d'évaluation
- AUB - Microscopic Analysis of UrineDocument4 pagesAUB - Microscopic Analysis of UrineJeanne Rodiño100% (1)
- GIEEE TGMP Policy Terms For 2022-23Document5 pagesGIEEE TGMP Policy Terms For 2022-23Janardhan Reddy TPas encore d'évaluation
- Pathophysiology of Ischemic Stroke FinalDocument3 pagesPathophysiology of Ischemic Stroke FinalAcohCChao67% (3)
- International Rice Research Notes Vol.18 No.1Document69 pagesInternational Rice Research Notes Vol.18 No.1ccquintosPas encore d'évaluation
- Abnormalities Protein Synthesis 2Document7 pagesAbnormalities Protein Synthesis 2yori rafiadliPas encore d'évaluation
- 3E - Agustin, Anne Julia - Group 1 - Case 7,8Document5 pages3E - Agustin, Anne Julia - Group 1 - Case 7,8Anne Julia AgustinPas encore d'évaluation
- Corona Vacsine 2nd DoseDocument2 pagesCorona Vacsine 2nd Doseavishekbhowmick18Pas encore d'évaluation
- Orthobullets Foot and AnkleDocument88 pagesOrthobullets Foot and AnkleStevent Richardo100% (1)
- Eaves Nickolas A 201211 MASc ThesisDocument69 pagesEaves Nickolas A 201211 MASc Thesisrajeev50588Pas encore d'évaluation
- FlaxDocument9 pagesFlaxXeeshan Rafique MirzaPas encore d'évaluation
- Biology Viral DiseasesDocument11 pagesBiology Viral DiseasesPrasoon Singh RajputPas encore d'évaluation
- NURSING CARE PLAN - Decreased Cardiac OutputDocument2 pagesNURSING CARE PLAN - Decreased Cardiac OutputRy Pablo83% (41)
- Aluminum in Co Ffee: AccessDocument9 pagesAluminum in Co Ffee: AccessJohnPas encore d'évaluation
- Adobe Scan Jul 28, 2023Document6 pagesAdobe Scan Jul 28, 2023Krishna ChaurasiyaPas encore d'évaluation
- NW NSC GR 10 Life Sciences p1 Eng Nov 2019Document12 pagesNW NSC GR 10 Life Sciences p1 Eng Nov 2019lunabileunakhoPas encore d'évaluation
- Subjective: Diarrhea Related To Watery Short Term: IndependentDocument4 pagesSubjective: Diarrhea Related To Watery Short Term: IndependentEmma Lyn SantosPas encore d'évaluation
- Sample Questionnaire For Understanding The Self: For Private Use OnlyDocument6 pagesSample Questionnaire For Understanding The Self: For Private Use Onlyirene ilustrisimo100% (1)
- 24 Bio Fertilization of BananaDocument6 pages24 Bio Fertilization of Bananamiceli57Pas encore d'évaluation
- Msds ChloroformDocument9 pagesMsds ChloroformAhmad ArisandiPas encore d'évaluation
- Malawi Clinical HIV Guidelines 2019 Addendumversion 8.1Document28 pagesMalawi Clinical HIV Guidelines 2019 Addendumversion 8.1INNOCENT KHULIWAPas encore d'évaluation