Vous aimerez peut-être aussi
- Basic EKG RefresherDocument210 pagesBasic EKG RefresherAaron D. Phoenix100% (6)
- Cardiovascular System PhysiologyDocument109 pagesCardiovascular System PhysiologyKing kakaPas encore d'évaluation
- 2011 ACLS PretestDocument19 pages2011 ACLS PretestAndrew HalimPas encore d'évaluation
- 2011 ACLS PretestDocument19 pages2011 ACLS PretestAndrew HalimPas encore d'évaluation
- ACLS Rhythms For The ACLS Algorithms: AppendixDocument32 pagesACLS Rhythms For The ACLS Algorithms: Appendixyan_ricci19100% (4)
- Cerebrovascular AccidentDocument26 pagesCerebrovascular AccidentMustafa Aadan100% (1)
- Repeat MD316 Written Paper August 2019Document14 pagesRepeat MD316 Written Paper August 2019Daniel Coyle100% (1)
- Acute Ischemic Stroke ManagementDocument38 pagesAcute Ischemic Stroke ManagementAndrio GultomPas encore d'évaluation
- 90,000 With AnswersDocument14 pages90,000 With AnswersHarsha Vipin100% (14)
- Oncologic Emergencies: Kristine P. Palisoc-Perez, MD Second Year ResidentDocument78 pagesOncologic Emergencies: Kristine P. Palisoc-Perez, MD Second Year Residentlady cuison100% (2)
- 2012 Near DrowningDocument35 pages2012 Near Drowningkamel6100% (1)
- Sepsis Update 2019Document44 pagesSepsis Update 2019Yeshwanth Umapathi100% (1)
- Cardiac BiomarkersDocument72 pagesCardiac BiomarkersAmey JatharPas encore d'évaluation
- NCP For HypertensionDocument1 pageNCP For Hypertensionrhizalyn1367% (6)
- AtlsDocument32 pagesAtlsMahesh RajwalPas encore d'évaluation
- LAS Science 9 Quarter 1 Week 1Document9 pagesLAS Science 9 Quarter 1 Week 1Jan Ice100% (1)
- Cals ReviewbjvjvjDocument14 pagesCals ReviewbjvjvjCarl Jay M Ocariza100% (1)
- Cardiac and Pulmonary Pre Block Anatomy Quiz QuestionsDocument12 pagesCardiac and Pulmonary Pre Block Anatomy Quiz Questionstlecesne100% (1)
- Biochemical Cardiac Markers in Acute Coronary Syndrome: by DR L A GovenderDocument43 pagesBiochemical Cardiac Markers in Acute Coronary Syndrome: by DR L A GovenderMichelle BandongPas encore d'évaluation
- Acute Coronary Syndromes: R Maharaj EmergencymedicineDocument64 pagesAcute Coronary Syndromes: R Maharaj EmergencymedicineMawar Eka PutriPas encore d'évaluation
- Acute Coronary SyndrommeDocument50 pagesAcute Coronary SyndrommeAndriani Kemala SariPas encore d'évaluation
- P ('t':'3', 'I':'669636497') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document56 pagesP ('t':'3', 'I':'669636497') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Muna NadiPas encore d'évaluation
- Acute Coronary Syndrome - YMDocument64 pagesAcute Coronary Syndrome - YMNirwanaPas encore d'évaluation
- Pharmacotherapy for ACS ManagementDocument71 pagesPharmacotherapy for ACS ManagementABREHAM BUKULOPas encore d'évaluation
- DR Mustika Mahbubi SPJP FIHA-How To Treat Acute Coronary Sydrome (STEMI Patient) in Pre and Post HospitalDocument59 pagesDR Mustika Mahbubi SPJP FIHA-How To Treat Acute Coronary Sydrome (STEMI Patient) in Pre and Post HospitalHiszom AsyhariPas encore d'évaluation
- Pathophysiology/Epidemiology of Acute Coronary Syndromes: 1 2 November 2019Document15 pagesPathophysiology/Epidemiology of Acute Coronary Syndromes: 1 2 November 2019anasPas encore d'évaluation
- Coronary Artery Disease Risk Factors and TreatmentDocument60 pagesCoronary Artery Disease Risk Factors and TreatmentliliPas encore d'évaluation
- ACS LectureDocument55 pagesACS LectureAyunda AlmiradaniPas encore d'évaluation
- Esc Acs GuidelinesDocument62 pagesEsc Acs GuidelineszakiyaPas encore d'évaluation
- 109890management StrokeDocument33 pages109890management StrokeGopi KrishnanPas encore d'évaluation
- Acute Miocard InfarkDocument32 pagesAcute Miocard InfarkhansPas encore d'évaluation
- Updates On Acute Coronary SyndromeDocument121 pagesUpdates On Acute Coronary SyndromeDwi Akbarina YahyaPas encore d'évaluation
- DR Vito Vascular ApicdDocument32 pagesDR Vito Vascular ApicdluckyariadneePas encore d'évaluation
- Stable Ischemic HeartDocument217 pagesStable Ischemic HeartReda SoPas encore d'évaluation
- Diagnostic Approaches to Cardiogenic ShockDocument22 pagesDiagnostic Approaches to Cardiogenic ShockannisPas encore d'évaluation
- 2014 Aha/Acc Guidelines For The Management of Patients With Non-St-Elevation Acute Coronary SyndromeDocument10 pages2014 Aha/Acc Guidelines For The Management of Patients With Non-St-Elevation Acute Coronary Syndromefarah0001Pas encore d'évaluation
- Biomarkers For Myocardial Infarction, CVS BlockDocument13 pagesBiomarkers For Myocardial Infarction, CVS BlockGlucose DRglucosePas encore d'évaluation
- ACS Guide Provides Updates on Diagnosis, TreatmentDocument72 pagesACS Guide Provides Updates on Diagnosis, TreatmentYeyen Devyanti HandokoPas encore d'évaluation
- Acute Coronary Syndrome - July 2009Document66 pagesAcute Coronary Syndrome - July 2009humairahermanPas encore d'évaluation
- ACS Management in Pandemic EraDocument56 pagesACS Management in Pandemic EraFatmawati nersPas encore d'évaluation
- Pre Hospital and Initial Management of Acute CoronaryDocument33 pagesPre Hospital and Initial Management of Acute CoronaryYudo PradanaPas encore d'évaluation
- Acute Myocardial InfarctionDocument13 pagesAcute Myocardial InfarctionSajjad KabirPas encore d'évaluation
- Ucm 484611Document92 pagesUcm 484611jackytungadiPas encore d'évaluation
- Onco EmergenciesDocument26 pagesOnco EmergenciespedsoncoaiimsPas encore d'évaluation
- Acute Coronary Syndrome Acute MIDocument41 pagesAcute Coronary Syndrome Acute MIAmjad SobehPas encore d'évaluation
- Stabil Koronária Betegség Diagnózisa És Kezelése. Rizikó FelmérésDocument37 pagesStabil Koronária Betegség Diagnózisa És Kezelése. Rizikó FelmérésHardy VajkPas encore d'évaluation
- ST Segment Elevated Myocardiac Infarction (Stemi) ObjectivesDocument25 pagesST Segment Elevated Myocardiac Infarction (Stemi) ObjectivesWilliam Yap WLPas encore d'évaluation
- Pre-Operative Assessment of Cardiac Patients in Non Cardiac SurgeryDocument36 pagesPre-Operative Assessment of Cardiac Patients in Non Cardiac SurgeryKush SurejaPas encore d'évaluation
- Acute Coronary SyndromeDocument30 pagesAcute Coronary SyndromeEndar EszterPas encore d'évaluation
- Intensive Versus Moderate Lipid Lowering With Statins After Acute Coronary SyndromesDocument43 pagesIntensive Versus Moderate Lipid Lowering With Statins After Acute Coronary Syndromeskjrunner2Pas encore d'évaluation
- DIAGNOSE AND TREAT ACUTE SEVERE HYPOTENSIONDocument49 pagesDIAGNOSE AND TREAT ACUTE SEVERE HYPOTENSIONDiana SabrinaPas encore d'évaluation
- Transient Ischemic AttackDocument23 pagesTransient Ischemic AttackAnonymous 9xHTwHYPas encore d'évaluation
- Pathogenesis of Cardiac DisordersDocument28 pagesPathogenesis of Cardiac DisordersUdochukwu EnebePas encore d'évaluation
- ACS Recognition ECG InterpretationDocument73 pagesACS Recognition ECG InterpretationJoel ChongPas encore d'évaluation
- Tugas DR Yoma AncaDocument30 pagesTugas DR Yoma Ancaaby mayuPas encore d'évaluation
- Newer Biomarkers of ACSDocument89 pagesNewer Biomarkers of ACSHafeesh FazuluPas encore d'évaluation
- ACS Lecture Derrick HuangDocument66 pagesACS Lecture Derrick HuangderrickPas encore d'évaluation
- Kelantan Guidelines For Nsteacs 2nd Edition 2012 PDFDocument48 pagesKelantan Guidelines For Nsteacs 2nd Edition 2012 PDFAhmad Nafais RahimiPas encore d'évaluation
- Acute Coronary SyndromeDocument16 pagesAcute Coronary SyndromeDr Hafashimana EmmanuelPas encore d'évaluation
- Blackshear - Chest Pain ContrastDocument13 pagesBlackshear - Chest Pain ContrastMazen SalamaPas encore d'évaluation
- Biochemical Makers of Cardiac DiseaseDocument45 pagesBiochemical Makers of Cardiac DiseaseSalman RashidPas encore d'évaluation
- Angina and MIDocument68 pagesAngina and MIAndrassy Twinkle AlineaPas encore d'évaluation
- Journal Presentation: Thrombin-Receptor Antagonist Vorapaxar in Acute Coronary SyndromesDocument16 pagesJournal Presentation: Thrombin-Receptor Antagonist Vorapaxar in Acute Coronary SyndromesStellaPas encore d'évaluation
- Acute Coronary SyndromeDocument41 pagesAcute Coronary SyndromeAbdulhameed MohamedPas encore d'évaluation
- Hemant Mahanand (201941103034) Case StudyDocument50 pagesHemant Mahanand (201941103034) Case StudyHemiPas encore d'évaluation
- Preoperative Evaluation AnesthesiaDocument27 pagesPreoperative Evaluation AnesthesiaDaniel Tanri RannuPas encore d'évaluation
- Acs SGD 8 - 20240308 - 051618 - 0000Document13 pagesAcs SGD 8 - 20240308 - 051618 - 0000Sarah JesikaPas encore d'évaluation
- Acute Coronary SyndromeDocument57 pagesAcute Coronary SyndromePreety ShresthaPas encore d'évaluation
- PENGGUNAAN OBAT PADA SISTEM CARDIOVASCULARDocument56 pagesPENGGUNAAN OBAT PADA SISTEM CARDIOVASCULARwidya vannesaPas encore d'évaluation
- CardiacDocument38 pagesCardiacMUHAMMAD ILHAMPas encore d'évaluation
- AHA Guidlines Grand Rounds CompressedDocument50 pagesAHA Guidlines Grand Rounds Compressedkamel6Pas encore d'évaluation
- ICUIntroResp PPSXDocument40 pagesICUIntroResp PPSXkamel6Pas encore d'évaluation
- Sinus Rhythms: Dysrhythmia Recognition & ManagementDocument29 pagesSinus Rhythms: Dysrhythmia Recognition & Managementkamel6Pas encore d'évaluation
- Airway Evaluation and Management2020Document21 pagesAirway Evaluation and Management2020kamel6Pas encore d'évaluation
- AHA Guidlines Grand Rounds CompressedDocument50 pagesAHA Guidlines Grand Rounds Compressedkamel6Pas encore d'évaluation
- NSR Parameters: 60 - 100 BPM Regular Normal 0.12 - 0.20 S 0.04 - 0.12 SDocument20 pagesNSR Parameters: 60 - 100 BPM Regular Normal 0.12 - 0.20 S 0.04 - 0.12 Skamel6Pas encore d'évaluation
- General Anaesthesia OverviewDocument21 pagesGeneral Anaesthesia Overviewkamel6Pas encore d'évaluation
- 0dbepropofol Study Orlando1Document34 pages0dbepropofol Study Orlando1kamel6Pas encore d'évaluation
- Adult Advanced Life Support (ALS)Document22 pagesAdult Advanced Life Support (ALS)JamestorsPas encore d'évaluation
- Advanced Airway Management Advanced Airway Management For The EMT For The EMT - Basic BasicDocument70 pagesAdvanced Airway Management Advanced Airway Management For The EMT For The EMT - Basic Basickamel6Pas encore d'évaluation
- ACLS DR YoungDocument64 pagesACLS DR YoungAnnie83DPas encore d'évaluation
- Abdomen 2 Anterior Abdominal Wall Part I (2005-2006)Document64 pagesAbdomen 2 Anterior Abdominal Wall Part I (2005-2006)kamel6Pas encore d'évaluation
- 5 Anesthesia For Trauma Patients, DR - Ho Opere, April2013Document18 pages5 Anesthesia For Trauma Patients, DR - Ho Opere, April2013kamel6Pas encore d'évaluation
- Anesthesia and Liver DiseasesDocument64 pagesAnesthesia and Liver Diseaseskamel6Pas encore d'évaluation
- Anesthetic Concerns in Renal FailureDocument16 pagesAnesthetic Concerns in Renal FailureEdwin Gustavo Sandoval TorresPas encore d'évaluation
- Anesthetic Concerns For The Patient With Renal and Hepatic DiseaseDocument43 pagesAnesthetic Concerns For The Patient With Renal and Hepatic Diseasekamel6Pas encore d'évaluation
- When You Can't Breathe, Nothing Else Matter: Presented by DR Parmeet BhatiaDocument140 pagesWhen You Can't Breathe, Nothing Else Matter: Presented by DR Parmeet Bhatiakamel6Pas encore d'évaluation
- Airway Management 1Document17 pagesAirway Management 1kamel6Pas encore d'évaluation
- Anesthetic Concerns For The Patient With Renal and Hepatic DiseaseDocument43 pagesAnesthetic Concerns For The Patient With Renal and Hepatic Diseasekamel6Pas encore d'évaluation
- 3 RegionalDocument21 pages3 Regionalkamel6Pas encore d'évaluation
- Anesthetic Concerns For The Patient With Renal and Hepatic DiseaseDocument43 pagesAnesthetic Concerns For The Patient With Renal and Hepatic Diseasekamel6Pas encore d'évaluation
- EcgDocument45 pagesEcgkamel6Pas encore d'évaluation
- 12 Acute Decompensated HFDocument36 pages12 Acute Decompensated HFFarida Nur AiniPas encore d'évaluation
- History & General ExamilationDocument82 pagesHistory & General Examilationkamel6Pas encore d'évaluation
- Jocs.15492 Articulo KozirevDocument7 pagesJocs.15492 Articulo KozirevCorazon MabelPas encore d'évaluation
- Nursing Care PlanDocument2 pagesNursing Care PlanHafza MacabatoPas encore d'évaluation
- Circulatory SystemDocument8 pagesCirculatory SystemstephaniecrossPas encore d'évaluation
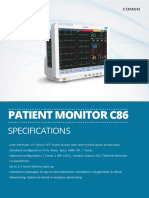
- Patient Monitor C86: SpecificationsDocument4 pagesPatient Monitor C86: SpecificationsBmet ConnectPas encore d'évaluation
- Arterial PunctureDocument14 pagesArterial PunctureGstayu WidiastutiPas encore d'évaluation
- Congestive Heart FailureDocument74 pagesCongestive Heart FailureNiharikaPas encore d'évaluation
- CPR Simulation Effect on Student MotivationDocument10 pagesCPR Simulation Effect on Student MotivationSherlLy TheoPas encore d'évaluation
- iFR Vs FFR For Guiding Coronary Revascularization - DEFINE-FLAIR (2 Year Results)Document32 pagesiFR Vs FFR For Guiding Coronary Revascularization - DEFINE-FLAIR (2 Year Results)rainmed USPas encore d'évaluation
- Reflective Writing 4Document2 pagesReflective Writing 4Luiza NiyazmetovaPas encore d'évaluation
- ECG ReadingDocument7 pagesECG ReadingEricka Lj Robles DimaculanganPas encore d'évaluation
- Kti Peredaran DarahDocument11 pagesKti Peredaran Darahdiki wahyudiPas encore d'évaluation
- Procedure For Patent Ductus Arteriosus (PDA) Device ClosureDocument13 pagesProcedure For Patent Ductus Arteriosus (PDA) Device ClosurejaganjaggiPas encore d'évaluation
- Laporan KematianDocument1 pageLaporan KematianIntan Robi'ahPas encore d'évaluation
- Body Fluids and CirculationDocument10 pagesBody Fluids and CirculationFree4TechPas encore d'évaluation
- Arteriovenous FistulaDocument11 pagesArteriovenous FistulaAbby GuiritanPas encore d'évaluation
- Echocardiography in Hypertrophic Cardiomyopathy Diagnosis, Prognosis, and Role in ManagementDocument6 pagesEchocardiography in Hypertrophic Cardiomyopathy Diagnosis, Prognosis, and Role in Managementjk045413Pas encore d'évaluation
- M2F Cardiovascular SystemDocument8 pagesM2F Cardiovascular SystemMeteor 858Pas encore d'évaluation
- First Aid Management of Haemorrhage: Veterinary Nursing JournalDocument3 pagesFirst Aid Management of Haemorrhage: Veterinary Nursing JournalRizqiPas encore d'évaluation
- ALFREDO 22010112130140 Lap - KTI Bab7Document19 pagesALFREDO 22010112130140 Lap - KTI Bab7titikPas encore d'évaluation
- مذكرة أم القرى - النسخة 3Document431 pagesمذكرة أم القرى - النسخة 3Nadreen OsmanPas encore d'évaluation
- Triglycerides Function and Impact on Heart HealthDocument5 pagesTriglycerides Function and Impact on Heart Healthrosidin_551390Pas encore d'évaluation
- Use of heparin in neurointervention literature reviewDocument6 pagesUse of heparin in neurointervention literature reviewStrawberry ShortcakePas encore d'évaluation
- Thyroid and HeartDocument6 pagesThyroid and HeartGaudeamus IgiturPas encore d'évaluation