Vous aimerez peut-être aussi
- CNS Stimulants DrugsDocument20 pagesCNS Stimulants DrugsDavid Jati MarintangPas encore d'évaluation
- Activity Overview ICSDocument2 pagesActivity Overview ICSDavid Jati MarintangPas encore d'évaluation
- Fluid, Buffer, Acid-Base Balance: Rondang SoegiantoDocument40 pagesFluid, Buffer, Acid-Base Balance: Rondang SoegiantoDavid Jati MarintangPas encore d'évaluation
- 72-Year-Old Man With Inferior Orbital Blow-Out Fracture: Erly, W. K. Et Al. Am. J. Roentgenol. 2003 180:1727-1730Document1 page72-Year-Old Man With Inferior Orbital Blow-Out Fracture: Erly, W. K. Et Al. Am. J. Roentgenol. 2003 180:1727-1730David Jati MarintangPas encore d'évaluation
- Biomembrane: Rondang R. Soegianto 2009Document11 pagesBiomembrane: Rondang R. Soegianto 2009David Jati MarintangPas encore d'évaluation
- 14.07.17 Kupang Sun McaDocument51 pages14.07.17 Kupang Sun McaDavid Jati MarintangPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Biopreservation and ProbioticsDocument11 pagesBiopreservation and ProbioticsDandapani Varsha100% (1)
- 2018 Insect Pest of Coconut Lect PDFDocument139 pages2018 Insect Pest of Coconut Lect PDFJohn Drei100% (1)
- Hand WashingDocument11 pagesHand Washinglo99988Pas encore d'évaluation
- PharmacologyDocument53 pagesPharmacologyapi-3743565Pas encore d'évaluation
- What If Ebook Top 10Document15 pagesWhat If Ebook Top 10Krishna TripathiPas encore d'évaluation
- Hepatitis B VaccineDocument4 pagesHepatitis B VaccineShantal AbelloPas encore d'évaluation
- Parts of The CellDocument2 pagesParts of The CellJess MCDPas encore d'évaluation
- Role of Digestive EnzymesDocument8 pagesRole of Digestive EnzymesvasaviPas encore d'évaluation
- NucleusDocument10 pagesNucleusPinak ChowdhuryPas encore d'évaluation
- Magnetic Pulse Therapy and Rife HealingDocument9 pagesMagnetic Pulse Therapy and Rife HealingHaSophim88% (8)
- The Human Genome - FinalDocument27 pagesThe Human Genome - FinalAbhi SachdevPas encore d'évaluation
- Molecular Targets of CNS TumorsDocument686 pagesMolecular Targets of CNS TumorsCherry_fPas encore d'évaluation
- Proteins in Serum & UrineDocument66 pagesProteins in Serum & Urinekiedd_04100% (1)
- Raza 2016Document12 pagesRaza 2016CARLOS ELOY ALARCON HOLGUINPas encore d'évaluation
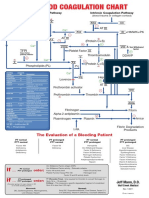
- Blood Clotting ChartDocument1 pageBlood Clotting ChartBianca SimionescuPas encore d'évaluation
- Science Quiz Bee Reviewer - High School LevelDocument6 pagesScience Quiz Bee Reviewer - High School LevelFamella GalmakPas encore d'évaluation
- HemophiliaDocument60 pagesHemophiliavibhurocksPas encore d'évaluation
- Hazard Identification - B-Sweet PotatoDocument2 pagesHazard Identification - B-Sweet PotatoFloreidPas encore d'évaluation
- Applications of Nutrigenomics in Animal Science1Document24 pagesApplications of Nutrigenomics in Animal Science1Ramachandran RamPas encore d'évaluation
- Genetics Essentials Concepts and Connections 3rd Edition Pierce Test BankDocument18 pagesGenetics Essentials Concepts and Connections 3rd Edition Pierce Test Bankkremswaiftexlh2l100% (29)
- Ch11 Lecture PPT ADocument50 pagesCh11 Lecture PPT ACamille Lopez50% (2)
- Republic of The Philippines Department of Education Region X Division of Bukidnon Quezon National High School Mibando, Quezon, BukidnonDocument13 pagesRepublic of The Philippines Department of Education Region X Division of Bukidnon Quezon National High School Mibando, Quezon, BukidnonSansen Diamante Colipano Jr.Pas encore d'évaluation
- 2021 Antagonistic Activity of Lactic Acid Bacteria Against Phytopathogenic Fungi Isolated From Cherry TomatoDocument10 pages2021 Antagonistic Activity of Lactic Acid Bacteria Against Phytopathogenic Fungi Isolated From Cherry TomatoEduardo Urbano Moraga CáceresPas encore d'évaluation
- Media Farmasi P.issn 0216-2083 E.issn 2622-0962 Vol. XV No. 1, April 2019Document6 pagesMedia Farmasi P.issn 0216-2083 E.issn 2622-0962 Vol. XV No. 1, April 2019Ivanda PrilsciliaPas encore d'évaluation
- Ddgi and Ddgdi RevDocument26 pagesDdgi and Ddgdi RevMarfu'ah Mar'ahPas encore d'évaluation
- Skeletal Muscle Omics Signatures in Cancer CachexiaDocument13 pagesSkeletal Muscle Omics Signatures in Cancer CachexiaMarina GomesPas encore d'évaluation
- Molecular Basis of InheritanceDocument8 pagesMolecular Basis of InheritancePriyanshu ShivamPas encore d'évaluation
- Analysis Prediction and Evaluation of CO PDFDocument6 pagesAnalysis Prediction and Evaluation of CO PDFSurfer LeoPas encore d'évaluation
- Test Bank For Microeconomics Canada in The Global Environment 8th Canadian Edition ParkinDocument24 pagesTest Bank For Microeconomics Canada in The Global Environment 8th Canadian Edition ParkinJesseRamseybrcn100% (39)
- Topic 8 - Grey MatterDocument53 pagesTopic 8 - Grey MatterStudent 365Pas encore d'évaluation