Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Click To Edit Master Title StyleDocument4 pagesClick To Edit Master Title StylemePas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Click To Edit Master Title StyleDocument4 pagesClick To Edit Master Title StyleSuluh Bayu WaskitoPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- 0561277Document8 pages0561277acutdevyPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- EndoftalmitisDocument14 pagesEndoftalmitisacutdevyPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- 555Document5 pages555acutdevyPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Bio Me Trike 89552023 A FullDocument11 pagesBio Me Trike 89552023 A FullacutdevyPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- BCR 3039Document12 pagesBCR 3039acutdevyPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Presentation TitleDocument2 pagesPresentation TitleacutdevyPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Destaque 18Document3 pagesDestaque 18acutdevyPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- bcr2831 PDFDocument9 pagesbcr2831 PDFacutdevyPas encore d'évaluation
- 1471 2407 12 41Document14 pages1471 2407 12 41acutdevyPas encore d'évaluation
- PDFDocument8 pagesPDFacutdevyPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Jurnal Kesehatan: by DffirentDocument5 pagesJurnal Kesehatan: by DffirentNindya Nur BagaskarinaPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Presendgsgstatio N Title: The Subheading Goes HereDocument4 pagesPresendgsgstatio N Title: The Subheading Goes HereacutdevyPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Presendgsgstatio N Title: The Subheading Goes HereDocument4 pagesPresendgsgstatio N Title: The Subheading Goes HereacutdevyPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- CATATAN Cek List Skill Lab3Document9 pagesCATATAN Cek List Skill Lab3acutdevyPas encore d'évaluation
- Tithuhdjhbdfjl EDocument2 pagesTithuhdjhbdfjl EacutdevyPas encore d'évaluation
- DTGDocument45 pagesDTGacutdevyPas encore d'évaluation
- Your Company InformationDocument2 pagesYour Company InformationacutdevyPas encore d'évaluation
- Mental Disorder Classification & Multiaxial Evaluation: Modified of Dr. Gitayanti Hadisukanto, SPKJ (K) 'SDocument49 pagesMental Disorder Classification & Multiaxial Evaluation: Modified of Dr. Gitayanti Hadisukanto, SPKJ (K) 'SacutdevyPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Hubungan Antara Pemberian Susu Formuladengan Kejadian Diare Pada Anak Usia 0-24 Bulandi Wilayah Kerja Puskesmas Balai Agung Sekayu TAHUN 2009Document8 pagesHubungan Antara Pemberian Susu Formuladengan Kejadian Diare Pada Anak Usia 0-24 Bulandi Wilayah Kerja Puskesmas Balai Agung Sekayu TAHUN 2009Andi Riezqa WulandariPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- NEUROPATIDocument16 pagesNEUROPATIFeby Vania OlliePas encore d'évaluation
- Metabolic Syndrome: Obesity Is The Central Problem: AbstrakDocument3 pagesMetabolic Syndrome: Obesity Is The Central Problem: Abstrakdies_vadisPas encore d'évaluation
- Child Neurology: Dr. Endang Mutiawati SP.SDocument28 pagesChild Neurology: Dr. Endang Mutiawati SP.SacutdevyPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Visum Et Repertum Pada Korban HidupDocument15 pagesVisum Et Repertum Pada Korban HidupEnda Athyyah Cahyani100% (1)
- Competence Standart: Understs The Farivius in Human SystemDocument5 pagesCompetence Standart: Understs The Farivius in Human SystemacutdevyPas encore d'évaluation
- Odds RatioDocument2 pagesOdds RatiokucinolenPas encore d'évaluation
- PARACETAMOL 120 MG/ 5 ML Pediatric Elixir: Pharmacological PropertiesDocument2 pagesPARACETAMOL 120 MG/ 5 ML Pediatric Elixir: Pharmacological PropertiesKarim FK MalahayatiPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Mental Disorder Classification & Multiaxial Evaluation: Modified of Dr. Gitayanti Hadisukanto, SPKJ (K) 'SDocument49 pagesMental Disorder Classification & Multiaxial Evaluation: Modified of Dr. Gitayanti Hadisukanto, SPKJ (K) 'SacutdevyPas encore d'évaluation
- Hancock1 109 - Hancock II Brochure - FinalDocument4 pagesHancock1 109 - Hancock II Brochure - FinalLuisaoPas encore d'évaluation
- Thromboangiitis ObliteransDocument5 pagesThromboangiitis Obliteransklinik mandiriPas encore d'évaluation
- (The European Society of Cardiology Series) Jose Luis Zamorano, Jeroen Bax, Juhani Knuuti, Patrizio Lancellotti, Fausto Pinto, Bogdan A. Popescu, Udo Sechtem - The ESC Textbook of Cardiovascular ImagiDocument865 pages(The European Society of Cardiology Series) Jose Luis Zamorano, Jeroen Bax, Juhani Knuuti, Patrizio Lancellotti, Fausto Pinto, Bogdan A. Popescu, Udo Sechtem - The ESC Textbook of Cardiovascular ImagiEdu MartinsPas encore d'évaluation
- Cardiovascular System ReviewDocument237 pagesCardiovascular System ReviewsenthilmnursePas encore d'évaluation
- Varicose Vein Causes Signs Symptoms TreatmentsDocument9 pagesVaricose Vein Causes Signs Symptoms TreatmentsFaizan SheikhPas encore d'évaluation
- (1 Bender, Et Al 2017) High Burden of Stroke Risk Factors in Developing Country The Case Study of BosniaDocument3 pages(1 Bender, Et Al 2017) High Burden of Stroke Risk Factors in Developing Country The Case Study of BosniasitialimahPas encore d'évaluation
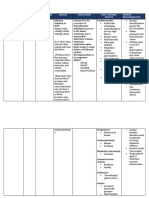
- Cues Nursing Diagnosis Objectives Nursing Interventions Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Objectives Nursing Interventions Rationale EvaluationHarvey Lampa SelimPas encore d'évaluation
- Ix StrokeDocument6 pagesIx StrokeWayne MacrohonPas encore d'évaluation
- Ascites in PoultryDocument37 pagesAscites in Poultryamamùra maamarPas encore d'évaluation
- EFNS Congress Vienna Semax AbstractDocument60 pagesEFNS Congress Vienna Semax AbstractnontjePas encore d'évaluation
- Mean Systemic Filling Pressure: Its Measurement and Meaning: ReviewDocument6 pagesMean Systemic Filling Pressure: Its Measurement and Meaning: ReviewAzharPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Ala 3Document30 pagesAla 3Alaz NellyPas encore d'évaluation
- CTO GuideDocument14 pagesCTO GuideTeodor BicaPas encore d'évaluation
- NursingDocument30 pagesNursingWilmaBongotanPadawilPas encore d'évaluation
- Purkinje Fibers of The Heart Conduction SystemDocument7 pagesPurkinje Fibers of The Heart Conduction SystemMark Norriel CajandabPas encore d'évaluation
- Leg Ulcer, What Do You Stand byDocument2 pagesLeg Ulcer, What Do You Stand byFree PizzaPas encore d'évaluation
- Roger Hainsworth (Auth.), Marek Malik (Eds.) - Clinical Guide To Cardiac Autonomic Tests-Springer Netherlands (1998)Document425 pagesRoger Hainsworth (Auth.), Marek Malik (Eds.) - Clinical Guide To Cardiac Autonomic Tests-Springer Netherlands (1998)Victor LaunePas encore d'évaluation
- 01 Cir 0000128521 02390 72Document8 pages01 Cir 0000128521 02390 72Petru GlavanPas encore d'évaluation
- Jurnal CT Cardiac 3Document27 pagesJurnal CT Cardiac 3Kakhfi Gemah PPas encore d'évaluation
- Coronarry Artery DiseaseDocument24 pagesCoronarry Artery DiseaseAriess897Pas encore d'évaluation
- Perilaku Pengendalian Hipertensi Pada Lansia - 1Document14 pagesPerilaku Pengendalian Hipertensi Pada Lansia - 1MessPas encore d'évaluation
- Advanced Textiles For Wound Compression 1Document24 pagesAdvanced Textiles For Wound Compression 1Ahsan NazirPas encore d'évaluation
- Drug Name Brand Name Classification Dosage Indications Side/ Adverse Effects Nursing ResponsibilitiesDocument2 pagesDrug Name Brand Name Classification Dosage Indications Side/ Adverse Effects Nursing ResponsibilitiesRonald BurkePas encore d'évaluation
- Language of Medicine 11th Edition Chabner Test BankDocument27 pagesLanguage of Medicine 11th Edition Chabner Test Bankajarinfecternl3vs100% (24)
- Asian Management of Hypertension: Current Status, Home Blood Pressure, and Specific Concerns in Philippines (A Country Report)Document4 pagesAsian Management of Hypertension: Current Status, Home Blood Pressure, and Specific Concerns in Philippines (A Country Report)DORINNE KINDAOPas encore d'évaluation
- RRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRDocument2 pagesRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRSaginesh MkPas encore d'évaluation
- Anatomy of Spleen: Research TitleDocument8 pagesAnatomy of Spleen: Research TitleOmar MohammedPas encore d'évaluation
- A01628 CH19Document36 pagesA01628 CH19Yannis ZoldenbergPas encore d'évaluation
- Anatomy Heart Homework (Due Mon. 3-9 1 or Tues. 3-10 2 /4) Vocabulary - Define The FollowingDocument2 pagesAnatomy Heart Homework (Due Mon. 3-9 1 or Tues. 3-10 2 /4) Vocabulary - Define The FollowingKameron WardPas encore d'évaluation
- Head and Neck Blood Supply and DrainageDocument11 pagesHead and Neck Blood Supply and DrainageHisham ChomanyPas encore d'évaluation
- Coloring Book for Adults & Grown Ups : An Easy & Quick Guide to Mastering Coloring for Stress Relieving Relaxation & Health Today!: The Stress Relieving Adult Coloring PagesD'EverandColoring Book for Adults & Grown Ups : An Easy & Quick Guide to Mastering Coloring for Stress Relieving Relaxation & Health Today!: The Stress Relieving Adult Coloring PagesÉvaluation : 2 sur 5 étoiles2/5 (12)
- Creative Abstract Watercolor: The beginner's guide to expressive and imaginative paintingD'EverandCreative Abstract Watercolor: The beginner's guide to expressive and imaginative paintingPas encore d'évaluation
- Art Models Ginger040: Figure Drawing Pose ReferenceD'EverandArt Models Ginger040: Figure Drawing Pose ReferenceÉvaluation : 4 sur 5 étoiles4/5 (5)
- One Zentangle a Day: A 6-Week Course in Creative Drawing for Relaxation, Inspiration, and FunD'EverandOne Zentangle a Day: A 6-Week Course in Creative Drawing for Relaxation, Inspiration, and FunÉvaluation : 4 sur 5 étoiles4/5 (25)
- The Everything Art Handbook: A Comprehensive Guide to More Than 100 Art Techniques and Tools of the TradeD'EverandThe Everything Art Handbook: A Comprehensive Guide to More Than 100 Art Techniques and Tools of the TradePas encore d'évaluation
- Sharpie Art Workshop: Techniques & Ideas for Transforming Your WorldD'EverandSharpie Art Workshop: Techniques & Ideas for Transforming Your WorldÉvaluation : 3 sur 5 étoiles3/5 (16)
- Portrait Painting in Oil: 10 Step by Step Guides from Old Masters: Learn to Paint Portraits via Detailed Oil Painting DemonstrationsD'EverandPortrait Painting in Oil: 10 Step by Step Guides from Old Masters: Learn to Paint Portraits via Detailed Oil Painting DemonstrationsÉvaluation : 4.5 sur 5 étoiles4.5/5 (3)
- Celestial Watercolor: Learn to Paint the Zodiac Constellations and Seasonal Night SkiesD'EverandCelestial Watercolor: Learn to Paint the Zodiac Constellations and Seasonal Night SkiesÉvaluation : 3.5 sur 5 étoiles3.5/5 (6)